

Effectiveness of de-implementation of low-value healthcare practices: an overview of systematic reviews
- PMID: 39103927
- PMCID: PMC11299416
- DOI: 10.1186/s13012-024-01384-6
Effectiveness of de-implementation of low-value healthcare practices: an overview of systematic reviews
Abstract
Background: Reducing low-value care (LVC) is crucial to improve the quality of patient care while increasing the efficient use of scarce healthcare resources. Recently, strategies to de-implement LVC have been mapped against the Expert Recommendation for Implementing Change (ERIC) compilation of strategies. However, such strategies' effectiveness across different healthcare practices has not been addressed. This overview of systematic reviews aimed to investigate the effectiveness of de-implementation initiatives and specific ERIC strategy clusters.
Methods: We searched MEDLINE (Ovid), Epistemonikos.org and Scopus (Elsevier) from 1 January 2010 to 17 April 2023 and used additional search strategies to identify relevant systematic reviews (SRs). Two reviewers independently screened abstracts and full texts against a priori-defined criteria, assessed the SR quality and extracted pre-specified data. We created harvest plots to display the results.
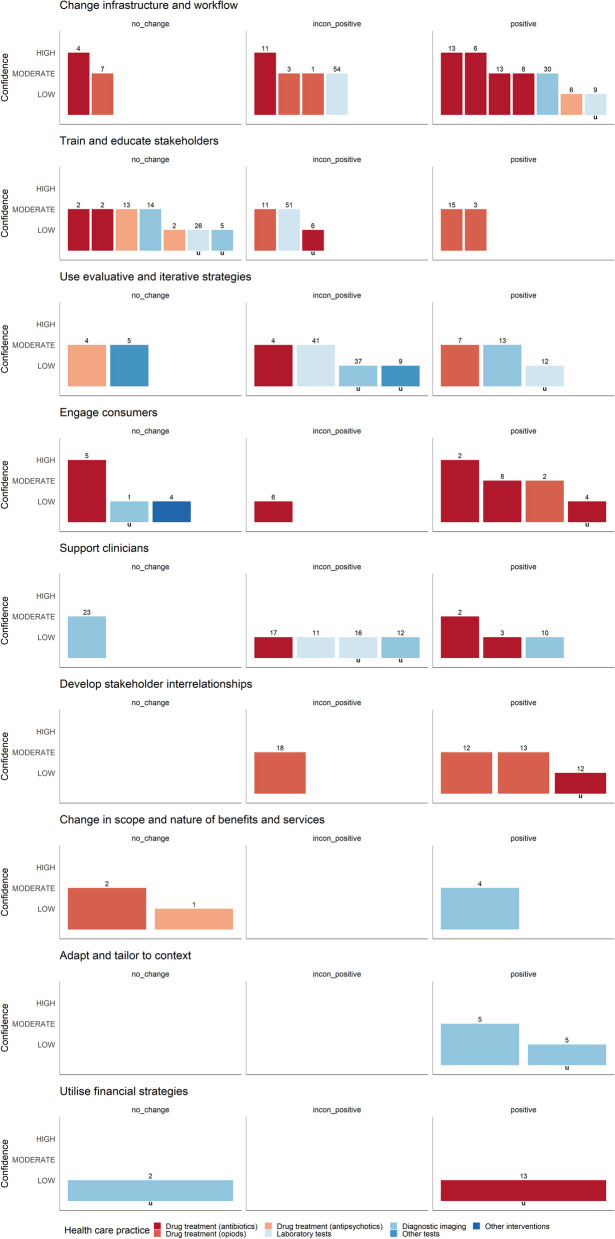
Results: Of 46 included SRs, 27 focused on drug treatments, such as antibiotics or opioids, twelve on laboratory tests or diagnostic imaging and seven on other healthcare practices. In categorising de-implementation strategies, SR authors applied different techniques: creating self-developed strategies (n = 12), focussing on specific de-implementation strategies (n = 14) and using published taxonomies (n = 12). Overall, 15 SRs provided evidence for the effectiveness of de-implementation interventions to reduce antibiotic and opioid utilisation. Reduced utilisation, albeit inconsistently significant, was documented in the use of antipsychotics and benzodiazepines, as well as in laboratory tests and diagnostic imaging. Strategies within the adapt and tailor to context, develop stakeholder interrelationships, and change infrastructure and workflow ERIC clusters led to a consistent reduction in LVC practices.
Conclusion: De-implementation initiatives were effective in reducing medication usage, and inconsistent significant reductions were observed for LVC laboratory tests and imaging. Notably, de-implementation clusters such as change infrastructure and workflow and develop stakeholder interrelationships emerged as the most encouraging avenues. Additionally, we provided suggestions to enhance SR quality, emphasising adherence to guidelines for synthesising complex interventions, prioritising appropriateness of care outcomes, documenting the development process of de-implementation initiatives and ensuring consistent reporting of applied de-implementation strategies.
Registration: OSF Open Science Framework 5ruzw.
Keywords: de-implementation; Antibiotic; Effectiveness; Laboratory tests; Low-value care; Overview of reviews.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
