

Imaging timing after surgery for glioblastoma: an evaluation of practice in Great Britain and Ireland (INTERVAL-GB)- a multi-centre, cohort study
- PMID: 39105956
- PMCID: PMC11341661
- DOI: 10.1007/s11060-024-04705-3
Imaging timing after surgery for glioblastoma: an evaluation of practice in Great Britain and Ireland (INTERVAL-GB)- a multi-centre, cohort study
Erratum in
-
Correction to: Imaging timing after surgery for glioblastoma: an evaluation of practice in Great Britain and Ireland (INTERVAL-GB)- a multi-centre, cohort study.J Neurooncol. 2025 Apr;172(2):495. doi: 10.1007/s11060-024-04924-8. J Neurooncol. 2025. PMID: 39976898 Free PMC article. No abstract available.
Abstract
Purpose: Post-operative MRI is used to assess extent of resection, monitor treatment response and detect progression in high-grade glioma. However, compliance with accepted guidelines for follow-up MRI, and impact on management/outcomes is unclear.
Methods: Multi-center, retrospective observational cohort study of patients with confirmed WHO grade 4 glioma (August 2018-February 2019) receiving oncological treatment.
Primary objective: investigate follow-up MRI surveillance practice and compliance with recommendations from NICE (Post-operative scan < 72h, MRI every 3-6 months) and EANO (Post-operative scan < 48h, MRI every 3 months).
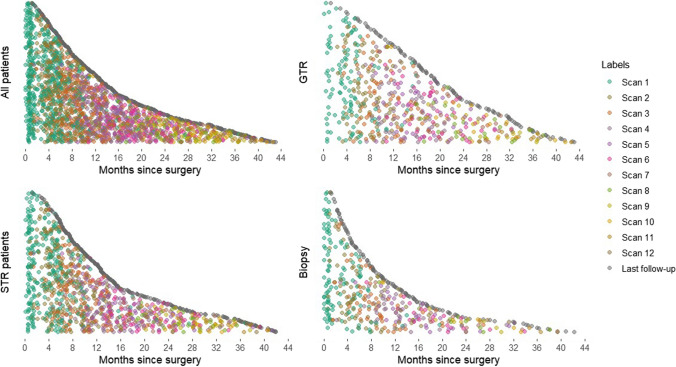
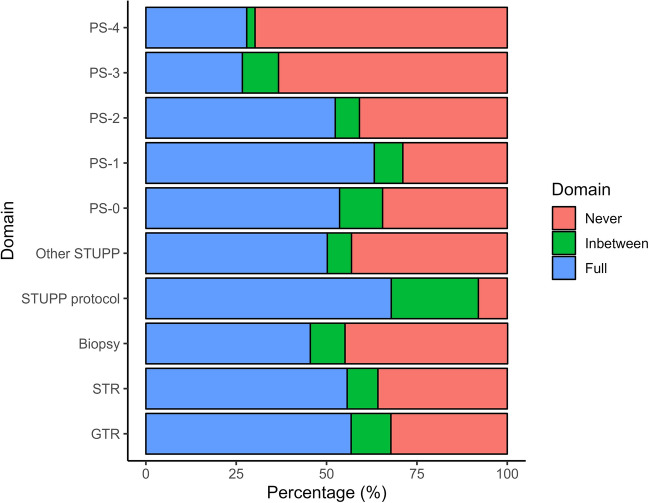
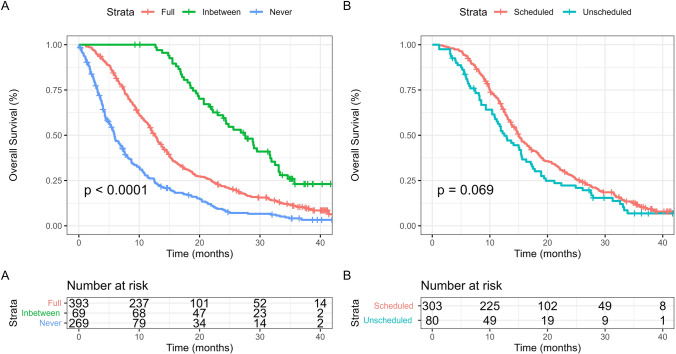
Results: There were 754 patients from 26 neuro-oncology centers with a median age of 63 years (IQR 54-70), yielding 10,100 (median, 12.5/person, IQR 5.2-19.4) person-months of follow-up. Of patients receiving debulking surgery, most patients had post-operative MRI within 72 h of surgery (78.0%, N = 407/522), and within 48 h of surgery (64.2%, N = 335/522). The median number of subsequent follow-up MRI scans was 1 (IQR 0-4). Compliance with NICE and EANO recommendations for follow-up MRI was 52.8% (N = 398/754) and 24.9% (N = 188/754), respectively. On multivariable Cox regression analysis, increased time spent in recommended follow-up according to NICE guidelines was associated with longer OS (HR 0.56, 95% CI 0.46-0.66, P < 0.001), but not PFS (HR 0.93, 95% CI 0.79-1.10, P = 0.349). Increased time spent in recommended follow-up according to EANO guidelines was associated with longer OS (HR 0.54, 95% CI 0.45-0.63, P < 0.001) but not PFS (HR 0.99, 95% CI 0.84-1.16, P = 0.874).
Conclusion: Regular surveillance follow-up for glioblastoma is associated with longer OS. Prospective trials are needed to determine whether regular or symptom-directed MRI influences outcomes.
Keywords: Glioblastoma; MRI; Neuro-oncology; Neuroimaging.
© 2024. The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
