

Comparison of two bundles for reducing surgical site infection in colorectal surgery: multicentre cohort study
- PMID: 39107075
- PMCID: PMC11303006
- DOI: 10.1093/bjsopen/zrae080
Comparison of two bundles for reducing surgical site infection in colorectal surgery: multicentre cohort study
Abstract
Background: There is controversy regarding the maximum number of elements that can be included in a surgical site infection prevention bundle. In addition, it is unclear whether a bundle of this type can be implemented at a multicentre level.
Methods: A pragmatic, multicentre cohort study was designed to analyse surgical site infection rates in elective colorectal surgery after the sequential implementation of two preventive bundle protocols. Secondary outcomes were to determine compliance with individual measures and to establish their effectiveness, duration of stay, microbiology and 30-day mortality rate.
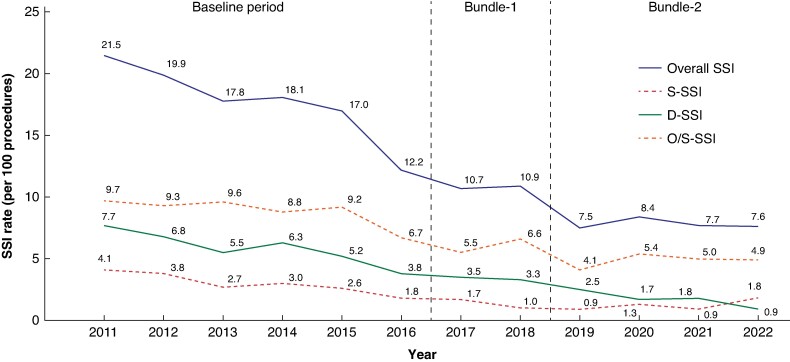
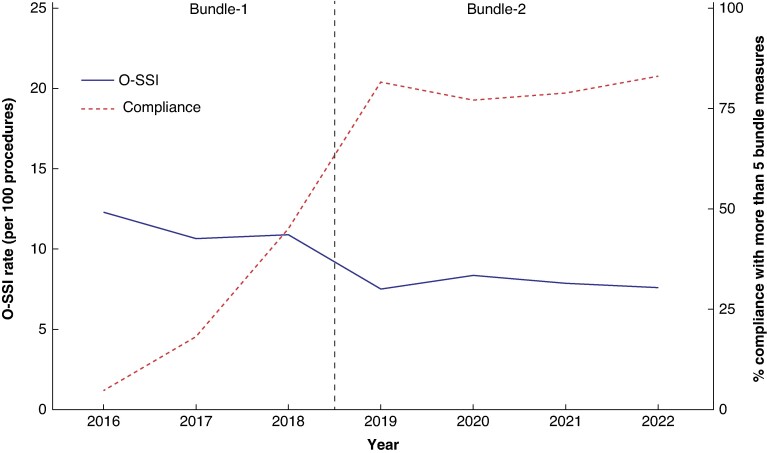
Results: A total of 32 205 patients were included. A 50% reduction in surgical site infection was achieved after the implementation of two sequential sets of bundles: from 18.16% in the Baseline group to 10.03% with Bundle-1 and 8.19% with Bundle-2. Bundle-2 reduced superficial-surgical site infection (OR 0.74 (95% c.i. 0.58 to 0.95); P = 0.018) and deep-surgical site infection (OR 0.66 (95% c.i. 0.46 to 0.93); P = 0.018) but not organ/space-surgical site infection (OR 0.88 (95% c.i. 0.74 to 1.06); P = 0.172). Compliance increased after the addition of four measures to Bundle-2. In the multivariable analysis, for organ/space-surgical site infection, laparoscopy, oral antibiotic prophylaxis and mechanical bowel preparation were protective factors in colonic procedures, while no protective factors were found in rectal surgery. Duration of stay fell significantly over time, from 7 in the Baseline group to 6 and 5 days for Bundle-1 and Bundle-2 respectively (P < 0.001). The mortality rate fell from 1.4% in the Baseline group to 0.59% and 0.6% for Bundle-1 and Bundle-2 respectively (P < 0.001). There was an increase in Gram-positive bacteria and yeast isolation, and reduction in Gram-negative bacteria and anaerobes in organ/space-surgical site infection.
Conclusions: The addition of measures to create a final 10-measure protocol had a cumulative protective effect on reducing surgical site infection. However, organ/space-surgical site infection did not benefit from the addition. No protective measures were found for organ/space-surgical site infection in rectal surgery. Compliance with preventive measures increased from Bundle-1 to Bundle-2.
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures
References
-
- European Centre for Disease Prevention and Control . Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals: 2011–2012. Stockholm: ECDC, 2013. https://www.ecdc.europa.eu/en/publications-data/surveillance-surgical-si... (accessed 13 August 2021)
-
- Gallego-Berciano P, Parra LM, Gallego-Munuera M, Cantero M, León-Gómez I, Sastre-García M et al. Encuesta de prevalencia de las infecciones relacionadas con la asistencia sanitaria y uso de antimicrobianos en los hospitales de España, 2022. Bol Epidemiol Semanal 2023;31:113–132
-
- de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control 2009;37:387–397 - PubMed
-
- Badia JM, Casey AL, Petrosillo N, Hudson PM, Mitchell SA, Crosby C. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect 2017;96:1–15 - PubMed
-
- Wick EC, Vogel JD, Church JM, Remzi F, Fazio VW. Surgical site infections in a ‘High Outlier’ institution: are colorectal surgeons to blame? Dis Colon Rectum 2009;52:374–379 - PubMed
