

This is a preprint.
Mass incarceration as a driver of the tuberculosis epidemic in Latin America and projected impacts of policy alternatives: A mathematical modeling study
- PMID: 39108530
- PMCID: PMC11302613
- DOI: 10.1101/2024.04.23.24306238
Mass incarceration as a driver of the tuberculosis epidemic in Latin America and projected impacts of policy alternatives: A mathematical modeling study
Update in
-
Mass incarceration as a driver of the tuberculosis epidemic in Latin America and projected effects of policy alternatives: a mathematical modelling study.Lancet Public Health. 2024 Nov;9(11):e841-e851. doi: 10.1016/S2468-2667(24)00192-0. Epub 2024 Oct 15. Lancet Public Health. 2024. PMID: 39419058 Free PMC article.
Abstract
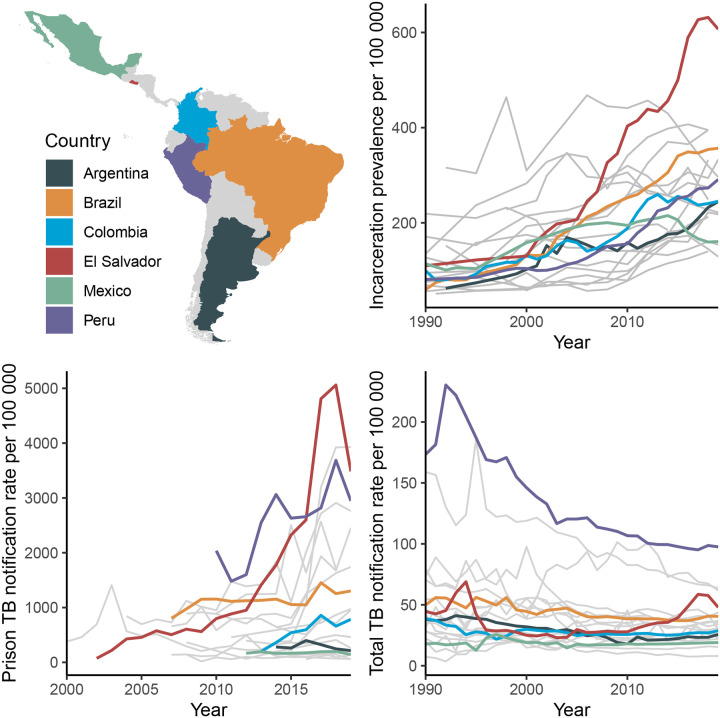
Background: Tuberculosis incidence is increasing in Latin America, where the incarcerated population has nearly quadrupled since 1990. The full impact of incarceration on the tuberculosis epidemic, accounting for effects beyond prisons, has never been quantified.
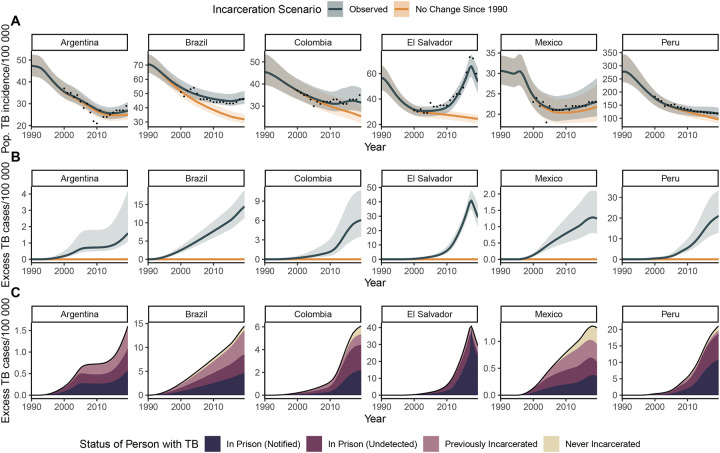
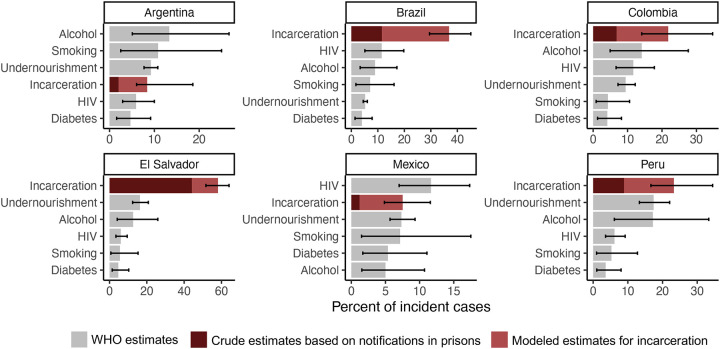
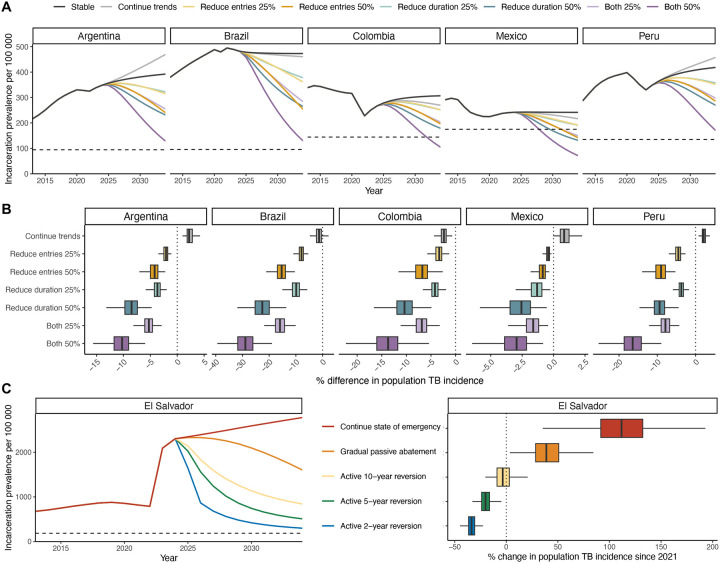
Methods: We calibrated dynamic compartmental transmission models to historical and contemporary data from Argentina, Brazil, Colombia, El Salvador, Mexico, and Peru, which comprise approximately 80% of the region's incarcerated population and tuberculosis burden. Using historical counterfactual scenarios, we estimated the transmission population attributable fraction (tPAF) for incarceration and the excess population-level burden attributable to increasing incarceration prevalence since 1990. We additionally projected the impact of alternative incarceration policies on future population tuberculosis incidence.
Findings: Population tuberculosis incidence in 2019 was 29.4% (95% UI, 23.9-36.8) higher than expected without the rise in incarceration since 1990, corresponding to 34,393 (95% UI, 28,295-42,579) excess incident cases across countries. The incarceration tPAF in 2019 was 27.2% (95% UI, 20.9-35.8), exceeding estimates for other risk factors like HIV, alcohol use disorder, and undernutrition. Compared to a scenario where incarceration rates remain stable at current levels, a gradual 50% reduction in prison admissions and duration of incarceration by 2034 would reduce population tuberculosis incidence by over 10% in all countries except Mexico.
Interpretation: The historical rise in incarceration in Latin America has resulted in a large excess tuberculosis burden that has been under-recognized to-date. International health agencies, ministries of justice, and national tuberculosis programs should collaborate to address this health crisis with comprehensive strategies, including decarceration.
Funding: National Institutes of Health.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
References
-
- Global Tuberculosis Report 2023: World Health Organization, 2023.
-
- Institute for Crime & Justice Policy Research. World Prison Brief. prisonstudies.org (accessed December 3 2023).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources