

Management of complications associated with percutaneous left atrial appendage closure with or without ablation: experience from 512 cases over a 4-year period
- PMID: 39108669
- PMCID: PMC11300201
- DOI: 10.3389/fcvm.2024.1388024
Management of complications associated with percutaneous left atrial appendage closure with or without ablation: experience from 512 cases over a 4-year period
Abstract
Background: Percutaneous left atrial appendage closure (LAAC) serves as an alternative prophylactic strategy for patients with non-valvular atrial fibrillation (AF) who cannot undergo anti-coagulation therapy. Proper management of associated complications is crucial to enhancing the procedure's success rate and mitigating perioperative risks and adverse events during follow-up.
Aims: This study aims to summarize our center's experience and strategies in managing procedural-related complications encountered in 512 cases of LAAC with or without ablation for AF conducted from January 2020 to December 2023.
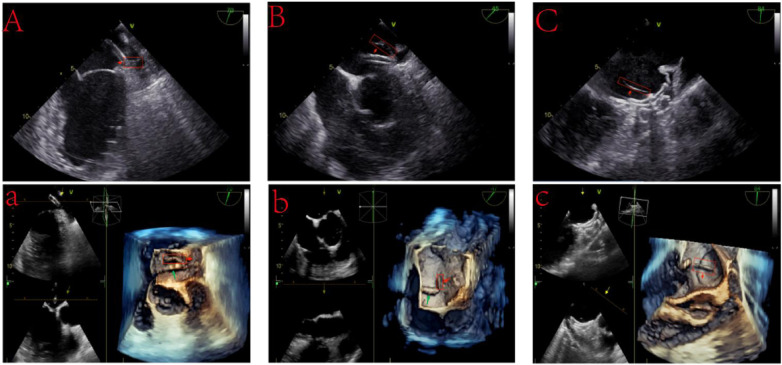
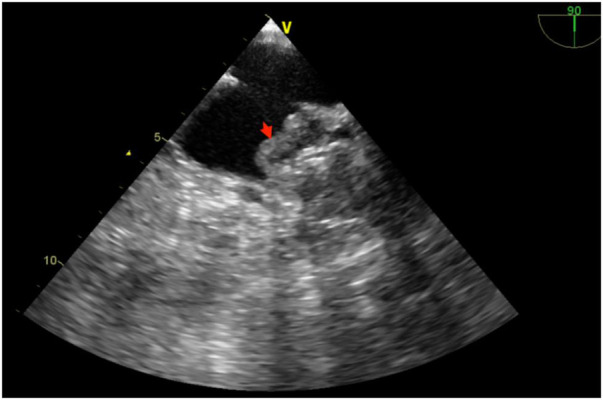
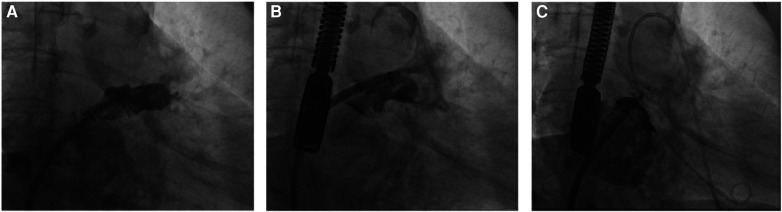
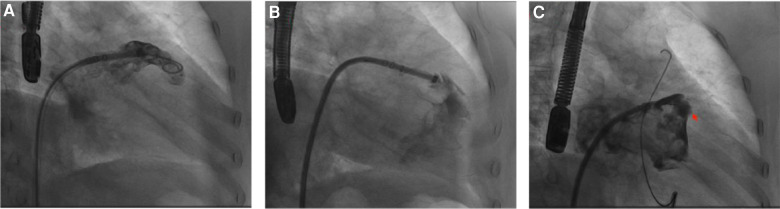
Results: We identified 11 significant intervention-requiring complications associated with LAAC with or without Ablation procedure. These included three cases of intraoperative thrombosis, three instances of pericardial effusion or tamponade, one case of device-related thrombosis, one peri-device leak, one systemic embolism, one bleeding episode, and one additional device-related complication. The categorization of intraoperative thrombosis was as follows: one patient exhibited heparin resistance; one experienced thrombosis due to prolonged device implantation during the LAAC with ablation procedure; and one had unexplained intraoperative thrombosis. The pericardial effusion or tamponade likely resulted from damage to the atrial appendage during LAAC device insertion. Two patients encountered device-related thrombosis and systemic embolism events possibly caused by non-standard postoperative antithrombotic medication use; one patient's peri-device leak may have resulted from incomplete endothelialization of the occluder post-surgery; one patient experienced postoperative bladder bleeding; and one patient's device-related complications occurred due to a dislodged strut frame that damaged the left atrial appendage, leading to pericardial effusion. Our proactive interventions enabled all patients with these surgical-related complications to be safely discharged, with subsequent follow-ups showing no adverse events.
Conclusion: Implementing targeted interventions for immediate procedural-related complications during the LAAC with or without ablation procedures enhances procedural success rates, diminishes postoperative mortality and patient disability, and bolsters stroke prevention efforts. This approach underscores the importance of a strategic response to complications, affirming the procedure's viability and safety in managing non-valvular AF in patients contraindicated for anticoagulation.
Keywords: atrial fibrillation; device-related thrombus; left atrial appendage closure; management strategy; procedural-related complications.
© 2024 Zou, Jiang, Lin, Yu, Li, Zhao, Hu and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Safety and feasibility of atrial fibrillation ablation after left atrial appendage closure: A single-center experience of the left atrial appendage closure first strategy.J Arrhythm. 2024 May 23;40(4):879-890. doi: 10.1002/joa3.13073. eCollection 2024 Aug. J Arrhythm. 2024. PMID: 39139871 Free PMC article.
-
Percutaneous left atrial appendage closure in patients with primary hemostasis disorders and atrial fibrillation.J Interv Card Electrophysiol. 2022 Aug;64(2):497-509. doi: 10.1007/s10840-021-01073-0. Epub 2021 Nov 25. J Interv Card Electrophysiol. 2022. PMID: 34822043
-
Should left atrial appendage closure be considered in resistant left atrial appendage thrombus cases? 'Former Foe, New Ally'.Pacing Clin Electrophysiol. 2024 Apr;47(4):583-590. doi: 10.1111/pace.14969. Epub 2024 Mar 13. Pacing Clin Electrophysiol. 2024. PMID: 38477017
-
Systematic review on left atrial appendage closure with the LAmbre device in patients with non-valvular atrial fibrillation.BMC Cardiovasc Disord. 2020 Feb 12;20(1):78. doi: 10.1186/s12872-020-01349-9. BMC Cardiovasc Disord. 2020. PMID: 32050904 Free PMC article.
-
Percutaneous left atrial appendage closure with the Watchman device: a systematic review.Postepy Kardiol Interwencyjnej. 2024 Mar;20(1):18-29. doi: 10.5114/aic.2024.136406. Epub 2024 Mar 15. Postepy Kardiol Interwencyjnej. 2024. PMID: 38616940 Free PMC article. Review.
Cited by
-
Left Atrial Appendage Closure With Catheter Ablation vs. Ablation Alone on Outcomes of Atrial Fibrillation in Heart Failure With Reduced Ejection Fraction: A Propensity Score-Matched Analysis.Cureus. 2024 Nov 27;16(11):e74577. doi: 10.7759/cureus.74577. eCollection 2024 Nov. Cureus. 2024. PMID: 39735150 Free PMC article.
References
-
- Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. Developed with the special contribution of the European heart rhythm association. Eur Heart J. (2012) 33:2719–47. 10.1093/eurheartj/ehs253 - DOI - PubMed
LinkOut - more resources
Full Text Sources