

Mitral Valve Prolapse With Mitral Annular Disjunction Causing Ventricular Tachycardia During a Stress Test: A Case Report
- PMID: 39109096
- PMCID: PMC11302552
- DOI: 10.7759/cureus.64020
Mitral Valve Prolapse With Mitral Annular Disjunction Causing Ventricular Tachycardia During a Stress Test: A Case Report
Abstract
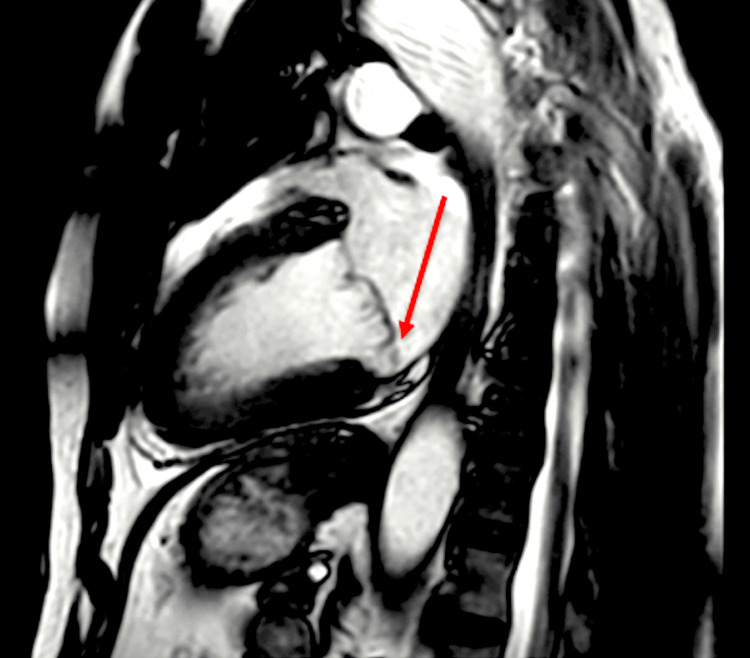
Mitral valve prolapse (MVP) is a relatively common valvular disorder characterized by displacement of one or both mitral valve leaflets into the left atrium (LA) during systole. Mitral annular disjunction (MAD) is an associated abnormality where a portion of the mitral valve annulus attaches superiorly in the left atrial wall. Although MVP is often considered benign, it can rarely lead to serious complications such as ventricular arrhythmias, especially when MAD is present. Herein, we present a case of a 63-year-old male with MVP and MAD who experienced sustained ventricular tachycardia (VT) during cardiac stress testing. This case underscores the importance of recognizing MVP with MAD as a potential substrate for ventricular arrhythmias, notably under heightened physiological or induced periods of stress.
Keywords: cardiac mri; cardiac stress test; mitral annular disjunction; mitral valve prolapse; ventricular tachycardia (vt).
Copyright © 2024, Palomino Abella et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Hospital Corporation of America (HCA) and the University of Central Florida (UCF) issued approval MS3293. This was reviewed by the HCA hospital research advisory committee, and all appropriate IRB forms were signed. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures








References
-
- Arrhythmic mitral valve prolapse and mitral annular disjunction: pathophysiology, risk stratification, and management. Essayagh B, Sabbag A, El-Am E, Cavalcante JL, Michelena HI, Enriquez-Sarano M. Eur Heart J. 2023;44:3121–3135. - PubMed
-
- Mitral valve prolapse, ventricular arrhythmias, and sudden death. Basso C, Iliceto S, Thiene G, Perazzolo Marra M. Circulation. 2019;140:952–964. - PubMed
-
- Imaging considerations and clinical implications of mitral annular disjunction. Drescher CS, Kelsey MD, Yankey GS, et al. Circ Cardiovasc Imaging. 2022;15:0. - PubMed
-
- Mitral annular disjunction: beyond mitral valve prolapse. Faria B, Ribeiro S, Calvo L, et al. Rev Port Cardiol. 2023;42:873–878. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous