

Race and Sex Differences in the Association of Bystander CPR for Cardiac Arrest
- PMID: 39109427
- PMCID: PMC11347084
- DOI: 10.1161/CIRCULATIONAHA.124.068732
Race and Sex Differences in the Association of Bystander CPR for Cardiac Arrest
Abstract
Background: Bystander cardiopulmonary resuscitation (CPR) is associated with higher survival for out-of-hospital cardiac arrest, but whether its association with survival differs by patients' sex and race and ethnicity is less clear.
Methods: Within a large US registry, we identified 623 342 nontraumatic out-of-hospital cardiac arrests during 2013 to 2022 for this observational cohort study. Using hierarchical logistic regression, we examined whether there was a differential association between bystander CPR and survival outcomes by patients' sex and race and ethnicity, overall and by neighborhood strata.
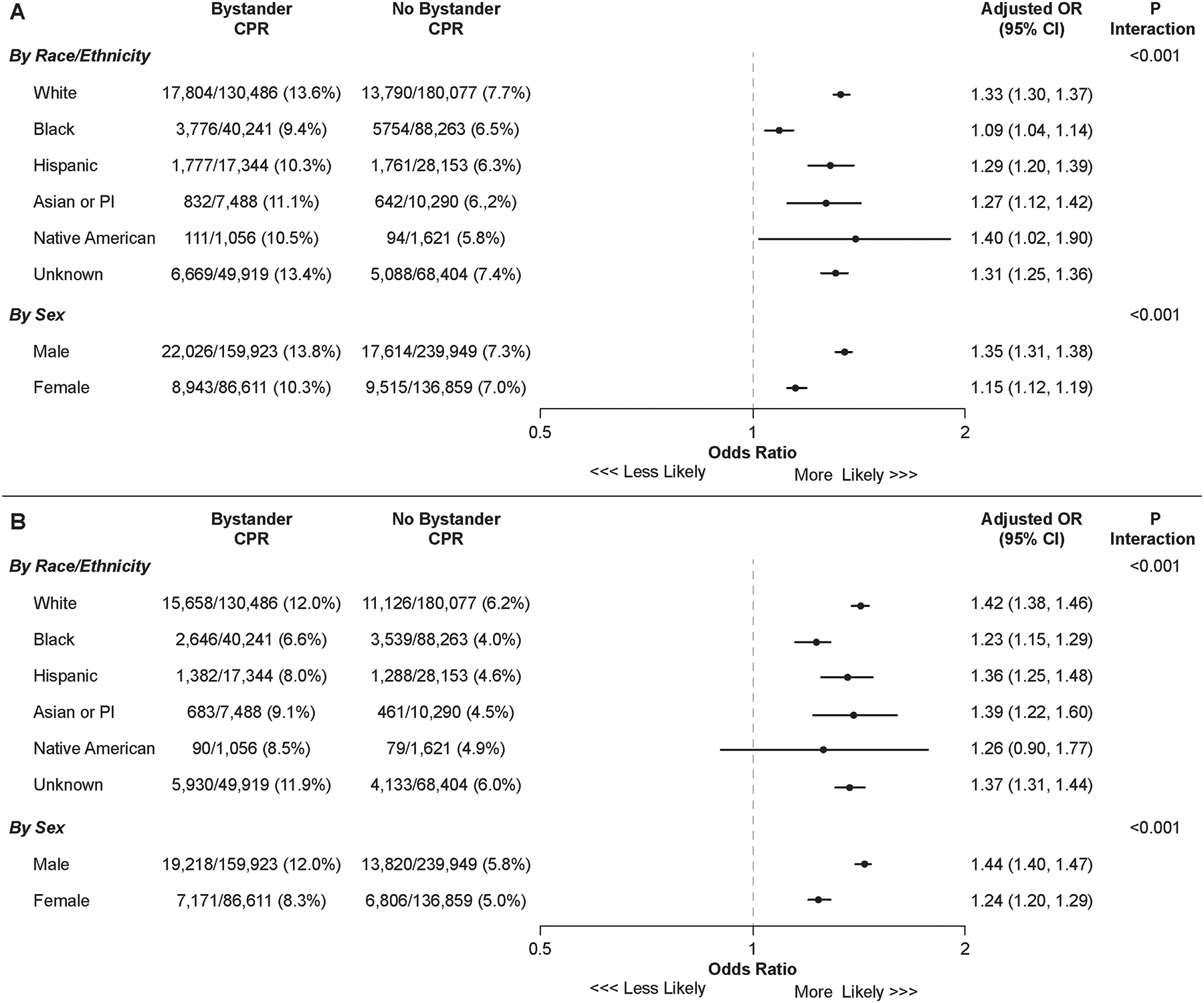
Results: Mean age was 62.1±17.1 years, and 35.9% were women. Nearly half of patients (49.8%) were non-Hispanic White; 20.6% were non-Hispanic Black; 7.3% were Hispanic; 2.9% were Asian; and 0.4% were Native American. Overall, 58 098 (9.3%) survived to hospital discharge. Although bystander CPR was associated with higher survival in each race and ethnicity group, the association of bystander CPR compared with patients without bystander CPR in each racial and ethnic group was highest in individuals who were White (adjusted odds ratio [OR], 1.33 [95% CI, 1.30-1.37]) and Native American (adjusted OR, 1.40 [95% CI, 1.02-1.90]) and lowest in individuals who were Black (adjusted OR, 1.09 [95% CI, 1.04-1.14]; Pinteraction<0.001). The adjusted OR for bystander CPR compared with those without bystander CPR for Hispanic patients was 1.29 (95% CI, 1.20-1.139), for Asian patients, it was 1.27 (95% CI, 1.12-1.42), and for those of unknown race, it was 1.31 (95% CI, 1.25-1.36). Similarly, bystander CPR was associated with higher survival in both sexes, but its association with survival was higher in men (adjusted OR, 1.35 [95% CI, 1.31-1.38]) than women (adjusted OR, 1.15 [95% CI, 1.12-1.19]; Pinteraction<0.001). The weaker association of bystander CPR in Black individuals and women was consistent across neighborhood race and ethnicity and income strata. Similar results were observed for the outcome of survival without severe neurological deficits.
Conclusions: Although bystander CPR was associated with higher survival in all patients, its association with survival was weakest for Black individuals and women with out-of-hospital cardiac arrest.
Keywords: cardiopulmonary resuscitation; heart arrest; racial groups; sex; survival.
Conflict of interest statement
None.
Figures

References
-
- Wenzel V, Krismer AC, Arntz HR, Sitter H, Stadlbauer KH, Lindner KH. A comparison of vasopressin and epinephrine for out-of-hospital cardiopulmonary resuscitation. N Engl J Med. 2004;350(2):105–113. - PubMed
-
- Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G, Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T, Dagnone E, Lyver M. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):647–656. - PubMed
-
- Hasselqvist-Ax I, Riva G, Herlitz J, Rosenqvist M, Hollenberg J, Nordberg P, Ringh M, Jonsson M, Axelsson C, Lindqvist J, Karlsson T, Svensson L. Early cardiopulmonary resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2015;372(24):2307–2315. - PubMed
-
- Kragholm K, Wissenberg M, Mortensen RN, Hansen SM, Malta Hansen C, Thorsteinsson K, Rajan S, Lippert F, Folke F, Gislason G, Kober L, Fonager K, Jensen SE, Gerds TA, Torp-Pedersen C, Rasmussen BS. Bystander Efforts and 1-Year Outcomes in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2017;376(18):1737–1747. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
