

Amyloid-Related Imaging Abnormalities in the Era of Anti-Amyloid Beta Monoclonal Antibodies for Alzheimer's Disease: Recent Updates on Clinical and Imaging Features and MRI Monitoring
- PMID: 39109501
- PMCID: PMC11306001
- DOI: 10.3348/kjr.2024.0105
Amyloid-Related Imaging Abnormalities in the Era of Anti-Amyloid Beta Monoclonal Antibodies for Alzheimer's Disease: Recent Updates on Clinical and Imaging Features and MRI Monitoring
Abstract
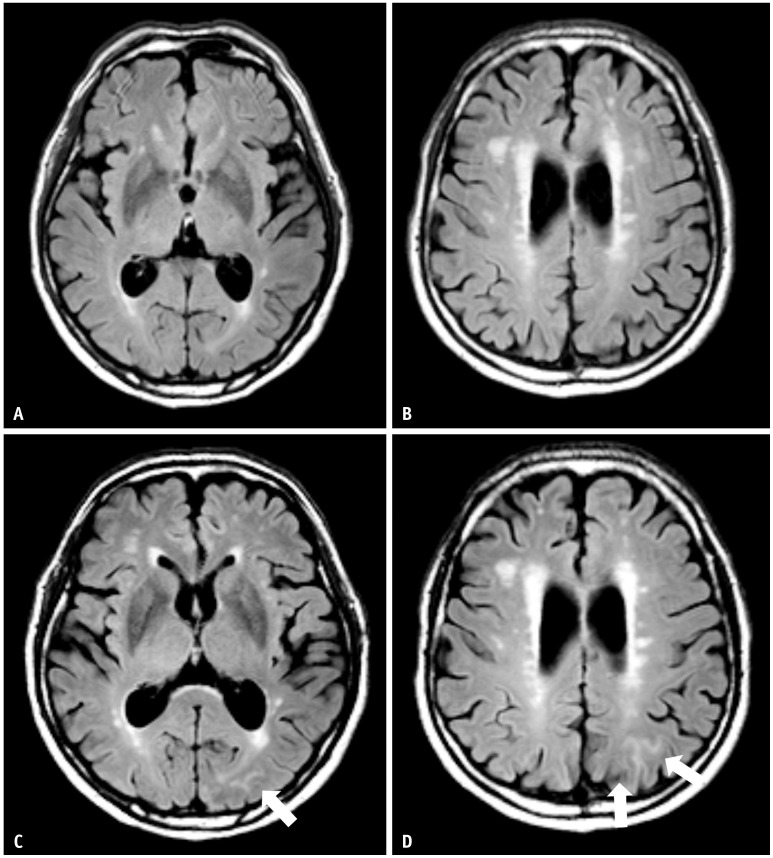
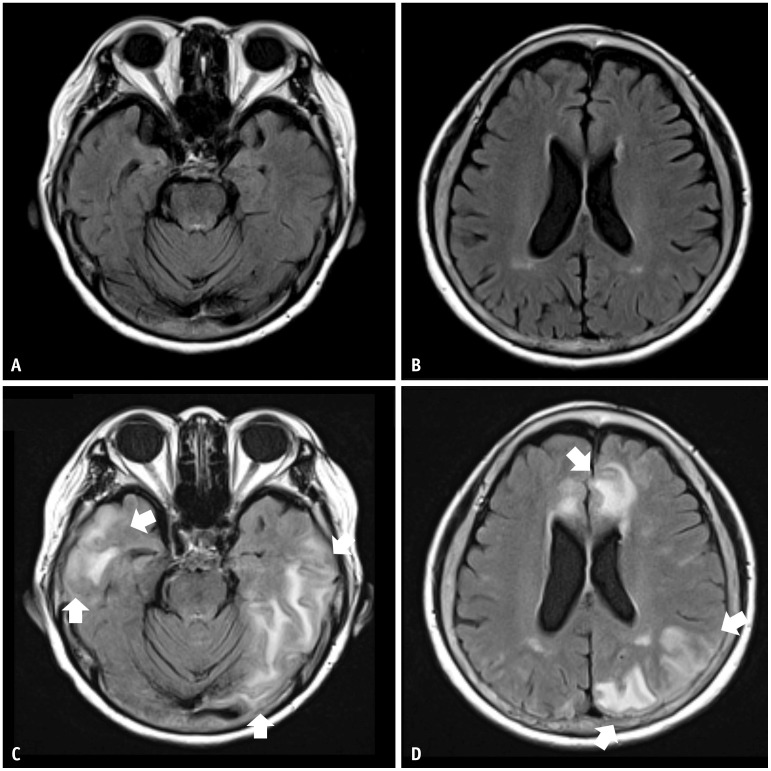
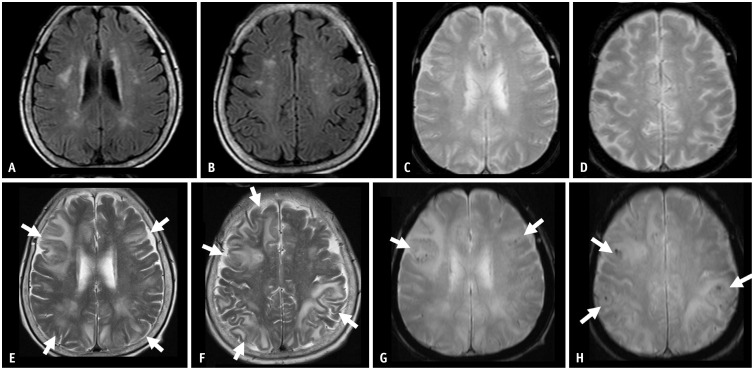
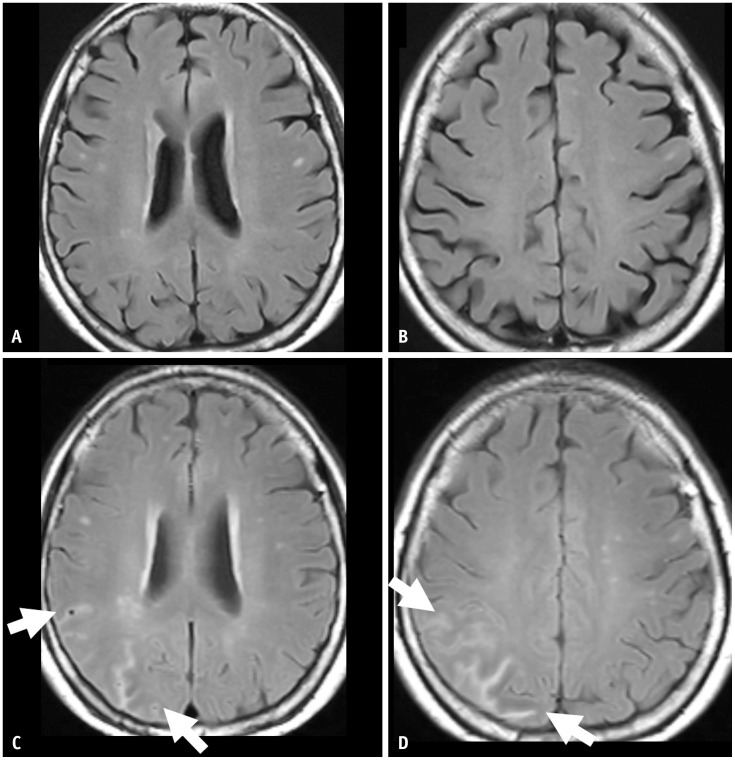
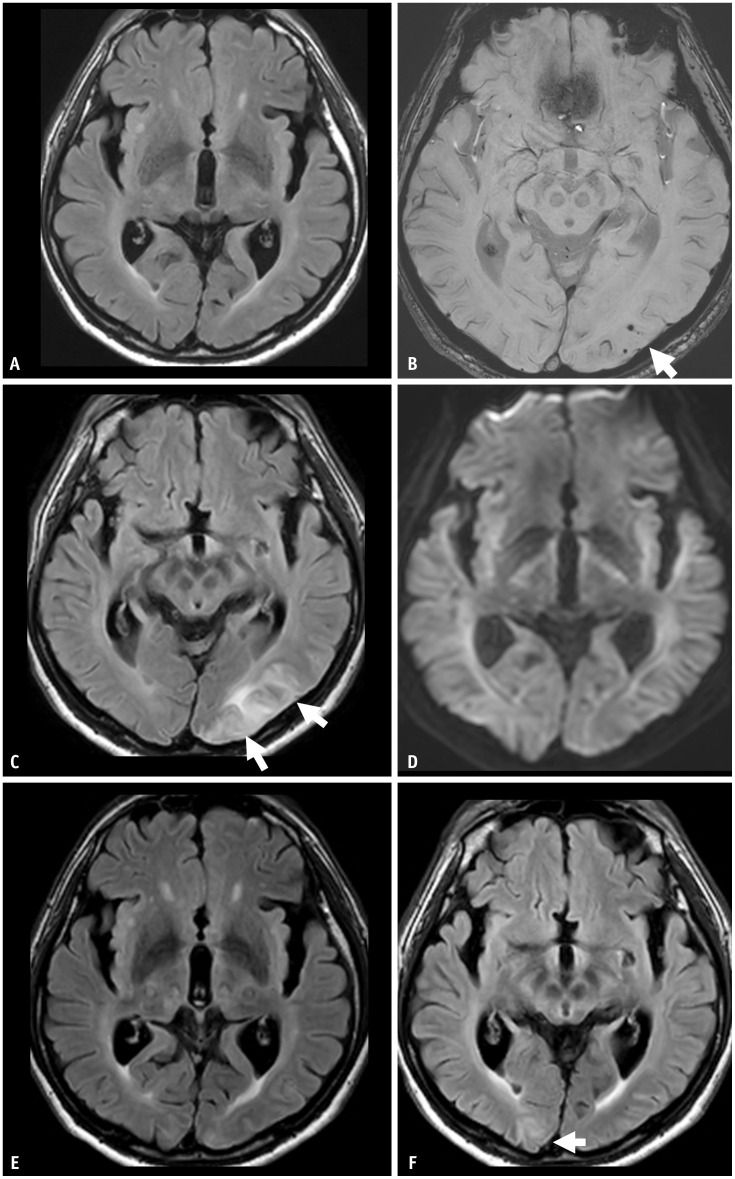
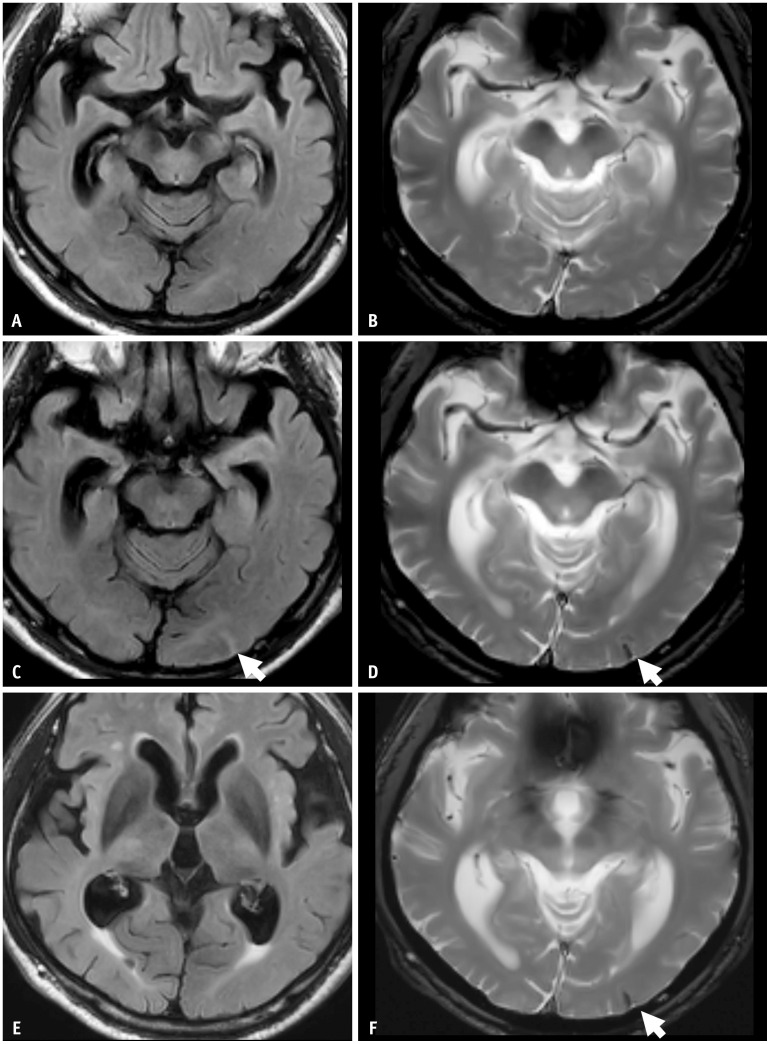
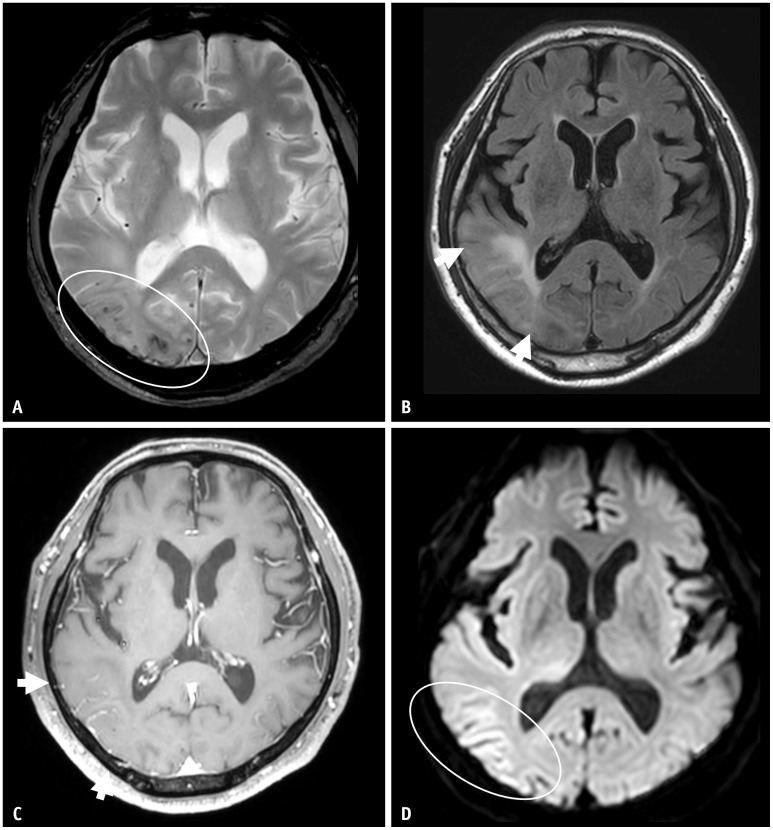
Recent advancements in Alzheimer's disease treatment have focused on the elimination of amyloid-beta (Aβ) plaque, a hallmark of the disease. Monoclonal antibodies such as lecanemab and donanemab can alter disease progression by binding to different forms of Aβ aggregates. However, these treatments raise concerns about adverse effects, particularly amyloid-related imaging abnormalities (ARIA). Careful assessment of safety, especially regarding ARIA, is crucial. ARIA results from treatment-related disruption of vascular integrity and increased vascular permeability, leading to the leakage of proteinaceous fluid (ARIA-E) and heme products (ARIA-H). ARIA-E indicates treatment-induced edema or sulcal effusion, while ARIA-H indicates treatment-induced microhemorrhage or superficial siderosis. The minimum recommended magnetic resonance imaging sequences for ARIA assessment are T2-FLAIR, T2* gradient echo (GRE), and diffusion-weighted imaging (DWI). T2-FLAIR and T2* GRE are necessary to detect ARIA-E and ARIA-H, respectively. DWI plays a role in differentiating ARIA-E from acute to subacute infarcts. Physicians, including radiologists, must be familiar with the imaging features of ARIA, the appropriate imaging protocol for the ARIA workup, and the reporting of findings in clinical practice. This review aims to describe the clinical and imaging features of ARIA and suggest points for the timely detection and monitoring of ARIA in clinical practice.
Keywords: Amyloid-related imaging abnormalities; Magnetic resonance imaging; Monoclonal antibodies.
Copyright © 2024 The Korean Society of Radiology.
Conflict of interest statement
Chong Hyun Suh, who holds the respective position as Assistant to the Editor of the
Figures
References
-
- Karran E, De Strooper B. The amyloid hypothesis in Alzheimer disease: new insights from new therapeutics. Nat Rev Drug Discov. 2022;21:306–318. - PubMed
-
- Jeong SY, Suh CH, Shim WH, Lim JS, Lee JH, Kim SJ. Incidence of amyloid-related imaging abnormalities in patients with Alzheimer disease treated with anti-β-amyloid immunotherapy: a meta-analysis. Neurology. 2022;99:e2092–e2101. - PubMed
-
- Barakos J, Purcell D, Suhy J, Chalkias S, Burkett P, Marsica Grassi C, et al. Detection and management of amyloid-related imaging abnormalities in patients with Alzheimer’s disease treated with anti-amyloid beta therapy. J Prev Alzheimers Dis. 2022;9:211–220. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
