

Protein Intake and Mortality in Older Adults With Chronic Kidney Disease
- PMID: 39110456
- PMCID: PMC11307132
- DOI: 10.1001/jamanetworkopen.2024.26577
Protein Intake and Mortality in Older Adults With Chronic Kidney Disease
Abstract
Importance: Avoiding high protein intake in older adults with chronic kidney disease (CKD) may reduce the risk of kidney function decline, but whether it can be suboptimal for survival is not well known.
Objective: To estimate the associations of total, animal, and plant protein intake with all-cause mortality in older adults with mild or moderate CKD and compare the results to those of older persons without CKD.
Design, setting, and participants: Data from 3 cohorts (Study on Cardiovascular Health, Nutrition and Frailty in Older Adults in Spain 1 and 2 and the Swedish National Study on Aging and Care in Kungsholmen [in Sweden]) composed of community-dwelling adults 60 years or older were used. Participants were recruited between March 2001 and June 2017 and followed up for mortality from December 2021 to January 2024. Those with no information on diet or mortality, with CKD stages 4 or 5, or undergoing kidney replacement therapy and kidney transplant recipients were excluded. Data were originally analyzed from June 2023 to February 2024 and reanalyzed in May 2024.
Exposures: Cumulative protein intake, estimated via validated dietary histories and food frequency questionnaires.
Main outcomes and measures: The study outcome was 10-year all-cause mortality, ascertained with national death registers. Chronic kidney disease was ascertained according to estimated glomerular filtration rates, urine albumin excretion, and diagnoses from medical records.
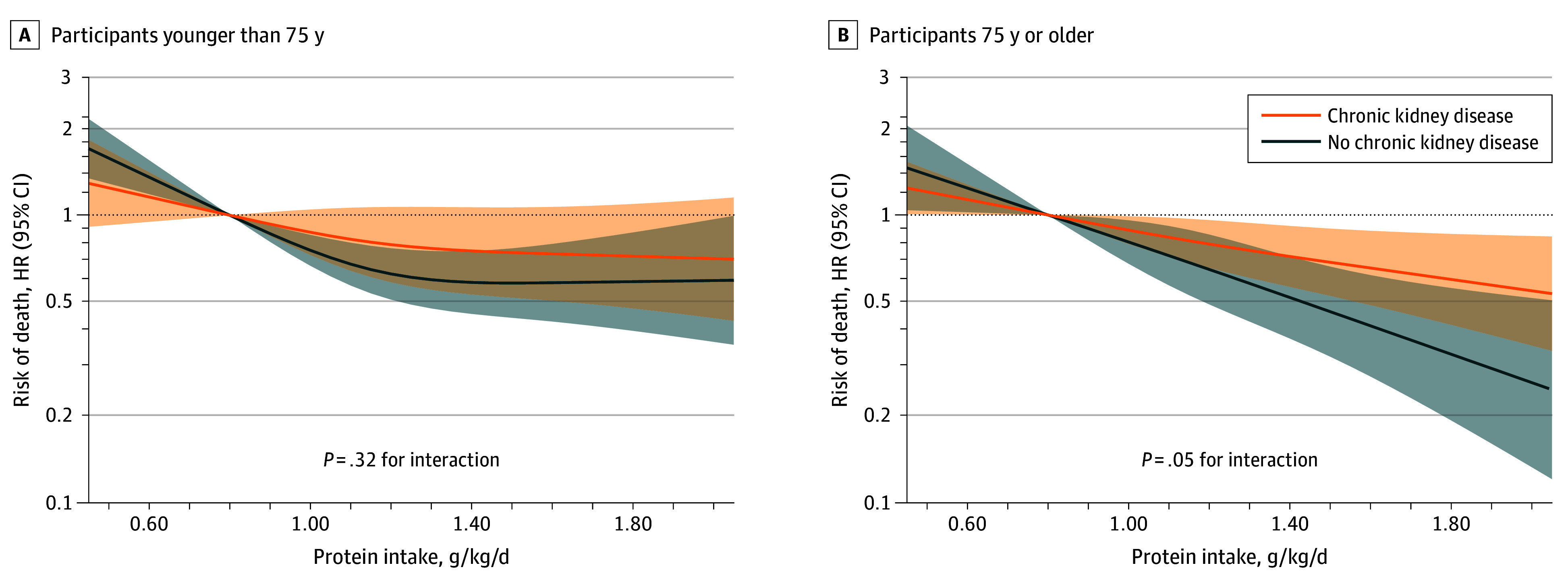
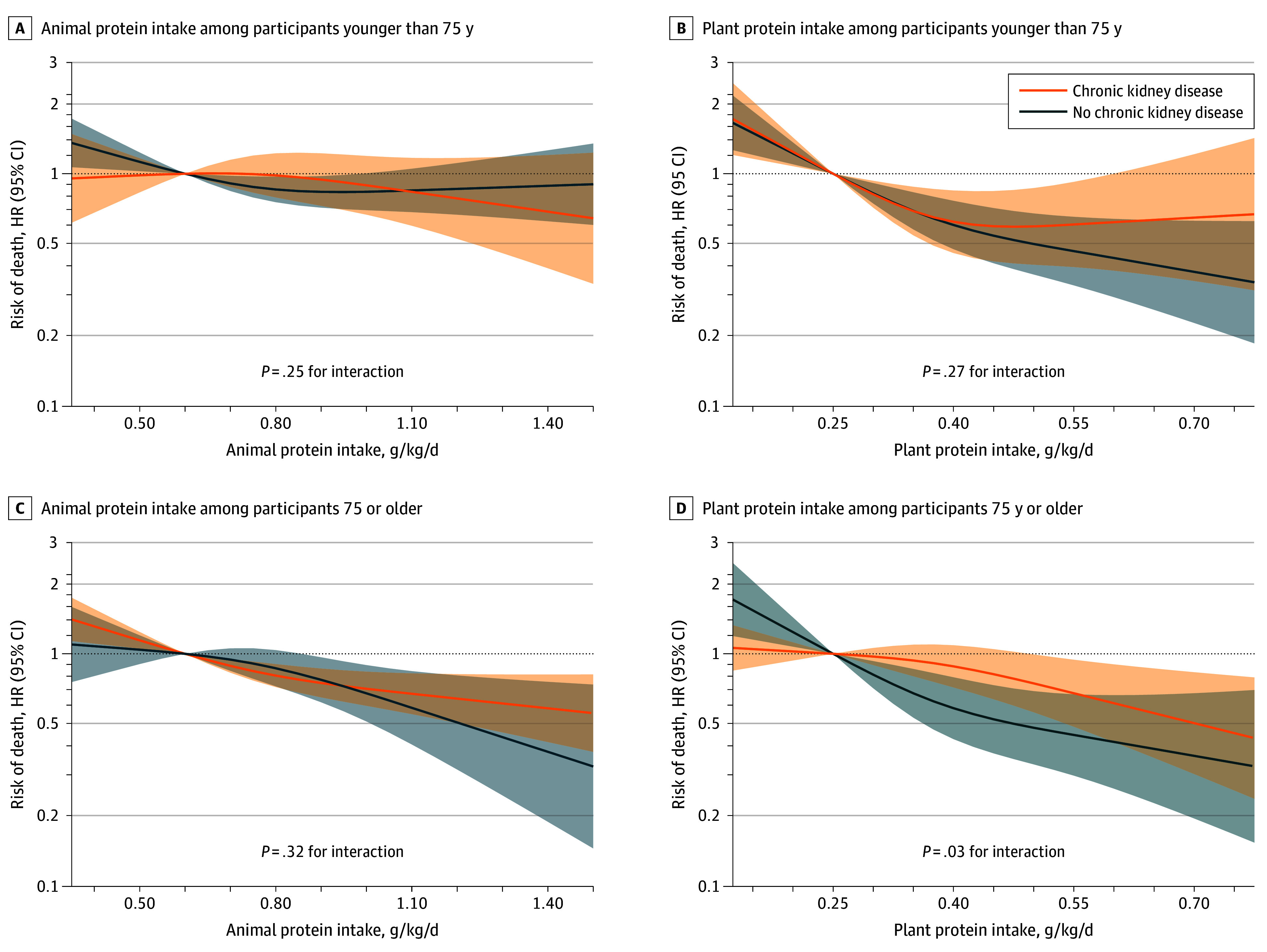
Results: The study sample consisted of 8543 participants and 14 399 observations. Of the 4789 observations with CKD stages 1 to 3, 2726 (56.9%) corresponded to female sex, and mean (SD) age was 78.0 (7.2) years. During the follow-up period, 1468 deaths were recorded. Higher total protein intake was associated with lower mortality among participants with CKD; adjusted hazard ratio (HR) for 1.00 vs 0.80 g/kg/d was 0.88 (95% CI, 0.79-0.98); for 1.20 vs 0.80 g/kg/d, 0.79 (95% CI, 0.66-0.95); and for 1.40 vs 0.80 g/kg/d, 0.73 (95% CI, 0.57-0.92). Associations with mortality were comparable for plant and animal protein (HRs, 0.80 [95% CI, 0.65-0.98] and 0.88 [95% CI, 0.81-0.95] per 0.20-g/kg/d increment, respectively) and for total protein intake in participants younger than 75 years vs 75 years or older (HRs, 0.94 [95% CI, 0.85-1.04] and 0.91 [95% CI, 0.85-0.98] per 0.20-g/kg/d increment in total protein intake, respectively). However, the hazards were lower among participants without CKD than in those with CKD (HRs, 0.85 [95% CI, 0.79-0.92] and 0.92 [95% CI, 0.86-0.98] per 0.20-g/kg/d increment, respectively; P = .02 for interaction).
Conclusions and relevance: In this multicohort study of older adults, higher intake of total, animal, and plant protein was associated with lower mortality in participants with CKD. Associations were stronger in those without CKD, suggesting that the benefits of proteins may outweigh the downsides in older adults with mild or moderate CKD.
Conflict of interest statement
Figures
References
-
- Piccoli GB, Cederholm T, Avesani CM, et al. . Nutritional status and the risk of malnutrition in older adults with chronic kidney disease—implications for low protein intake and nutritional care: a critical review endorsed by ERN-ERA and ESPEN. Clin Nutr. 2023;42(4):443-457. doi:10.1016/j.clnu.2023.01.018 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
