

Continuous Monitoring of Heart Rate Variability in Free-Living Conditions Using Wearable Sensors: Exploratory Observational Study
- PMID: 39110968
- PMCID: PMC11339560
- DOI: 10.2196/53977
Continuous Monitoring of Heart Rate Variability in Free-Living Conditions Using Wearable Sensors: Exploratory Observational Study
Abstract
Background: Wearable physiological monitoring devices are promising tools for remote monitoring and early detection of potential health changes of interest. The widespread adoption of such an approach across communities and over long periods of time will require an automated data platform for collecting, processing, and analyzing relevant health information.
Objective: In this study, we explore prospective monitoring of individual health through an automated data collection, metrics extraction, and health anomaly analysis pipeline in free-living conditions over a continuous monitoring period of several months with a focus on viral respiratory infections, such as influenza or COVID-19.
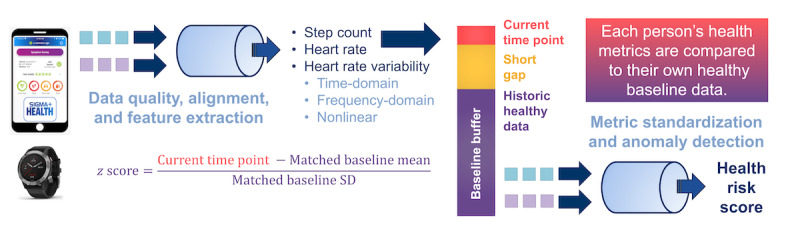
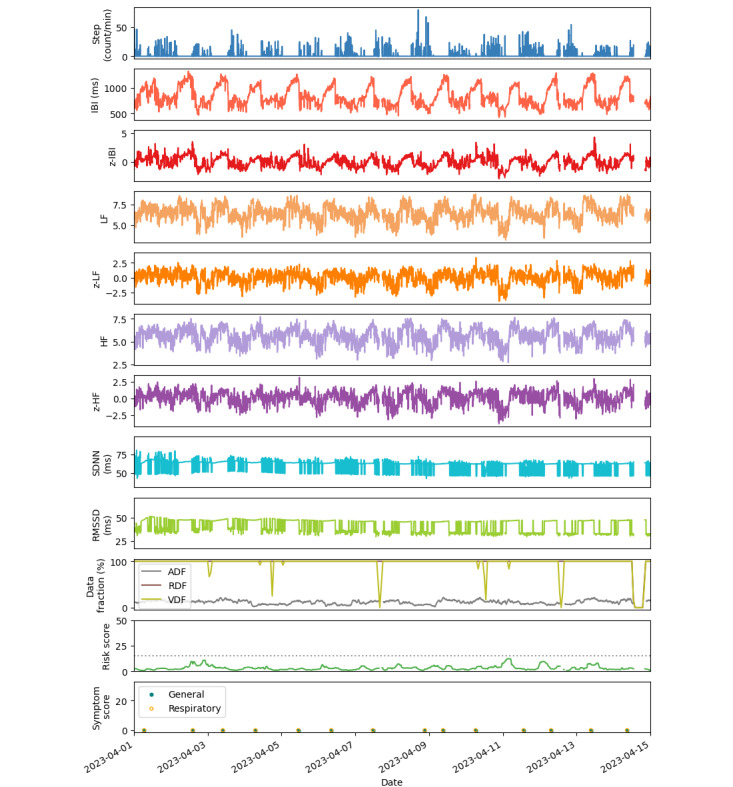
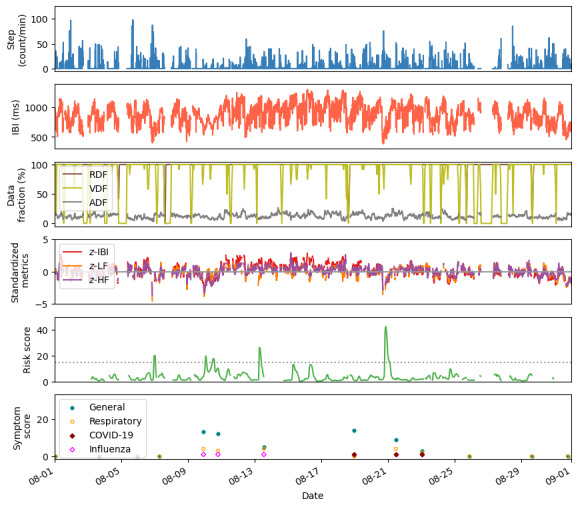
Methods: A total of 59 participants provided smartwatch data and health symptom and illness reports daily over an 8-month window. Physiological and activity data from photoplethysmography sensors, including high-resolution interbeat interval (IBI) and step counts, were uploaded directly from Garmin Fenix 6 smartwatches and processed automatically in the cloud using a stand-alone, open-source analytical engine. Health risk scores were computed based on a deviation in heart rate and heart rate variability metrics from each individual's activity-matched baseline values, and scores exceeding a predefined threshold were checked for corresponding symptoms or illness reports. Conversely, reports of viral respiratory illnesses in health survey responses were also checked for corresponding changes in health risk scores to qualitatively assess the risk score as an indicator of acute respiratory health anomalies.
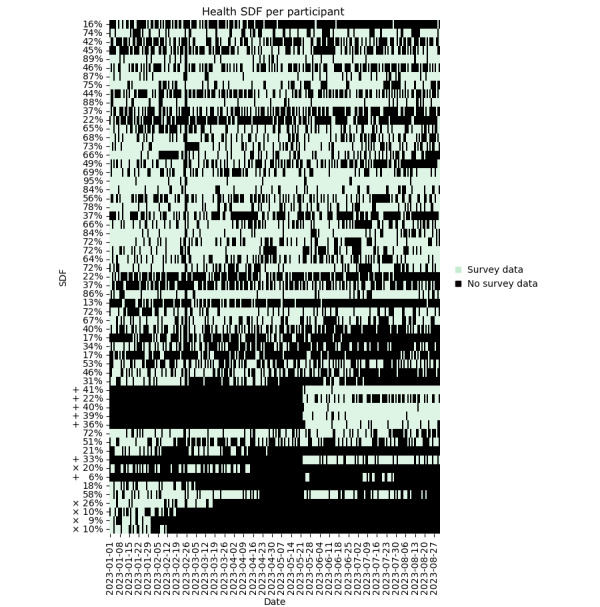
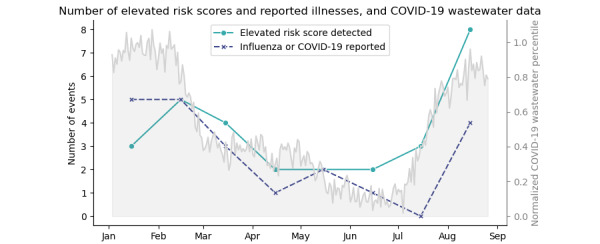
Results: The median average percentage of sensor data provided per day indicating smartwatch wear compliance was 70%, and survey responses indicating health reporting compliance was 46%. A total of 29 elevated health risk scores were detected, of which 12 (41%) had concurrent survey data and indicated a health symptom or illness. A total of 21 influenza or COVID-19 illnesses were reported by study participants; 9 (43%) of these reports had concurrent smartwatch data, of which 6 (67%) had an increase in health risk score.
Conclusions: We demonstrate a protocol for data collection, extraction of heart rate and heart rate variability metrics, and prospective analysis that is compatible with near real-time health assessment using wearable sensors for continuous monitoring. The modular platform for data collection and analysis allows for a choice of different wearable sensors and algorithms. Here, we demonstrate its implementation in the collection of high-fidelity IBI data from Garmin Fenix 6 smartwatches worn by individuals in free-living conditions, and the prospective, near real-time analysis of the data, culminating in the calculation of health risk scores. To our knowledge, this study demonstrates for the first time the feasibility of measuring high-resolution heart IBI and step count using smartwatches in near real time for respiratory illness detection over a long-term monitoring period in free-living conditions.
Keywords: PPG; community; data collection; data platform; devices; health risk; heart rate; heart rate variability; monitoring; observation study; photoplethysmography; physiological; physiological monitoring; remote monitoring; sensor; sensors; smartwatch; wearable; wearable devices; wearable sensors; wearables.
©Pooja Gaur, Dorota S Temple, Meghan Hegarty-Craver, Matthew D Boyce, Jonathan R Holt, Michael F Wenger, Edward A Preble, Randall P Eckhoff, Michelle S McCombs, Hope C Davis-Wilson, Howard J Walls, David E Dausch. Originally published in JMIR Formative Research (https://formative.jmir.org), 07.08.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Effects of Missing Data on Heart Rate Variability Measured From A Smartwatch: Exploratory Observational Study.JMIR Form Res. 2025 Feb 24;9:e53645. doi: 10.2196/53645. JMIR Form Res. 2025. PMID: 39993288 Free PMC article.
-
Physiological Sensors Equipped in Wearable Devices for Management of Long COVID Persisting Symptoms: Scoping Review.J Med Internet Res. 2025 Mar 26;27:e69506. doi: 10.2196/69506. J Med Internet Res. 2025. PMID: 40137051 Free PMC article.
-
Monitoring Health Care Workers at Risk for COVID-19 Using Wearable Sensors and Smartphone Technology: Protocol for an Observational mHealth Study.JMIR Res Protoc. 2021 May 12;10(5):e29562. doi: 10.2196/29562. JMIR Res Protoc. 2021. PMID: 33945497 Free PMC article.
-
Engagement and Participant Experiences With Consumer Smartwatches for Health Research: Longitudinal, Observational Feasibility Study.JMIR Mhealth Uhealth. 2020 Jan 29;8(1):e14368. doi: 10.2196/14368. JMIR Mhealth Uhealth. 2020. PMID: 32012078 Free PMC article.
-
The Accuracy of Wearable Photoplethysmography Sensors for Telehealth Monitoring: A Scoping Review.Telemed J E Health. 2023 Jun;29(6):813-828. doi: 10.1089/tmj.2022.0182. Epub 2022 Oct 25. Telemed J E Health. 2023. PMID: 36288566
References
-
- Massoomi MR, Handberg EM. Increasing and evolving role of smart devices in modern medicine. Eur Cardiol. 2019;14(3):181–186. doi: 10.15420/ecr.2019.02. https://europepmc.org/abstract/MED/31933689 - DOI - PMC - PubMed
-
- Haveman ME, van Rossum MC, Vaseur RME, van der Riet C, Schuurmann RCL, Hermens HJ, de Vries JPM, Tabak M. Continuous monitoring of vital signs with wearable sensors during daily life activities: validation study. JMIR Form Res. 2022;6(1):e30863. doi: 10.2196/30863. https://formative.jmir.org/2022/1/e30863/ v6i1e30863 - DOI - PMC - PubMed
-
- Esgalhado F, Batista A, Vassilenko V, Russo S, Ortigueira M. Peak detection and HRV feature evaluation on ECG and PPG signals. Symmetry. 2022;14(6):1139. doi: 10.3390/sym14061139. - DOI
LinkOut - more resources
Full Text Sources
