

A new, adaptive, self-administered, and generalizable method used to measure visual acuity
- PMID: 39110980
- PMCID: PMC11323045
- DOI: 10.1097/OPX.0000000000002160
A new, adaptive, self-administered, and generalizable method used to measure visual acuity
Abstract
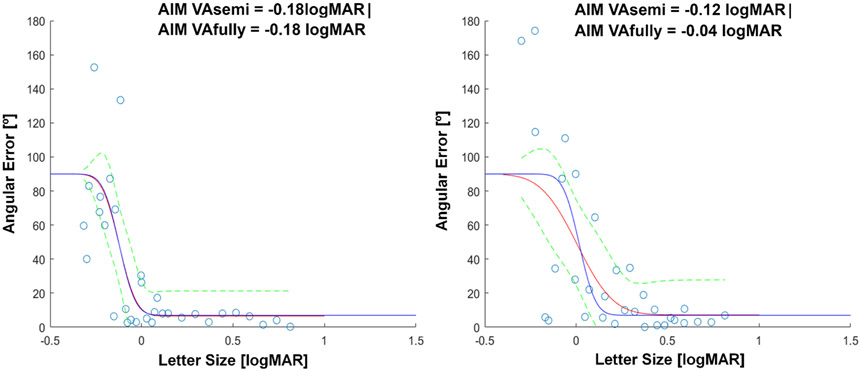
Significance: Angular Indication Measurement (AIM) is an adaptive, self-administered, and generalizable orientation-judgment method designed to interrogate visual functions. We introduce AIM Visual Acuity (VA) and show its features and outcome measures. Angular Indication Measurement VA's ability to detect defocus was comparable with that of an Early Treatment of Diabetic Retinopathy Study (ETDRS) letter chart and showed greater sensitivity to astigmatic blur.
Purpose: This proof-of-concept study introduces Angular Indication Measurement and applies it to VA.
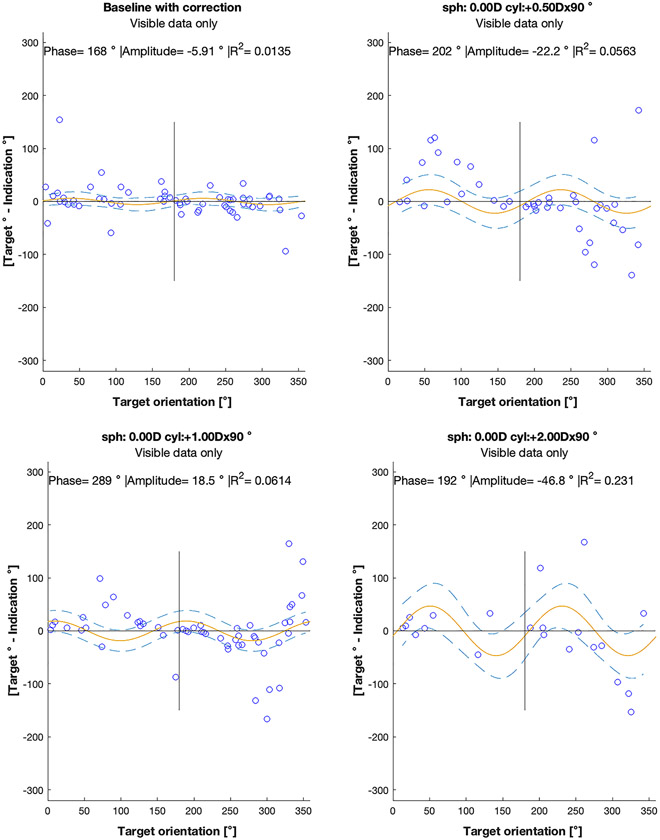
Methods: First, we compared the ability of AIM-VA and ETDRS to detect defocus and astigmatic blur in 22 normally sighted adults. Spherical and cylindrical lenses in the dominant eye induced blur. Second, we compared repeatability over two tests of AIM-VA and ETDRS.
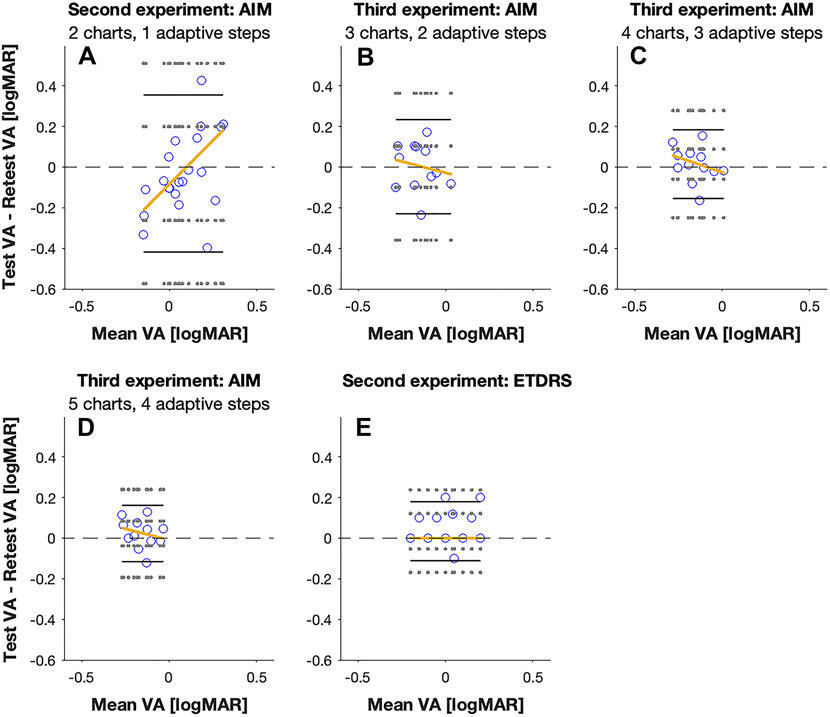
Results: A repeated-measure analysis of variance showed a main effect for defocus blur and test. For the astigmatism experiment, an interaction between blur and orientation was found. Pairwise comparisons showed that AIM was more sensitive to astigmatic-induced VA loss than ETDRS. Bland-Altman plots showed small bias and no systematic learning effect for either test type and improved repeatability with more than two adaptive steps for AIM-VA.
Conclusions: Angular Indication Measurement VA's ability to detect defocus was comparable with that of an ETDRS letter chart and showed greater sensitivity to induced astigmatic blur, and AIM-VA's repeatability is comparable with ETDRS when using two or more adaptive steps. Angular Indication Measurement's self-administered orientation judgment approach is generalizable to interrogate other visual functions, e.g., contrast, color, motion, and stereovision.
Copyright © 2024 American Academy of Optometry.
Conflict of interest statement
Conflict of Interest Disclosure: AIM is disclosed as patented (status pending during the time of submission) and held by Northeastern University, Boston, USA. JS and PJB are founders and shareholders of PerZeption Inc., which has an exclusive license agreement for AIM. All other authors declare no conflict of interests.
Figures








Update of
-
AIM (Angular Indication Measurement)- Visual Acuity: An adaptive, self-administered, and generalizable vision assessment method used to measure visual acuity.bioRxiv [Preprint]. 2023 Aug 15:2023.02.25.529586. doi: 10.1101/2023.02.25.529586. bioRxiv. 2023. Update in: Optom Vis Sci. 2024 Jul 1;101(7):451-463. doi: 10.1097/OPX.0000000000002160. PMID: 36909639 Free PMC article. Updated. Preprint.
References
-
- Raasch TW. Spherocylindrical refractive errors and visual acuity. Optom Vis Sci 1995;72:272–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
