

Myocardial Strain Measured by Cardiac Magnetic Resonance Predicts Cardiovascular Morbidity and Death
- PMID: 39111972
- PMCID: PMC11320766
- DOI: 10.1016/j.jacc.2024.05.050
Myocardial Strain Measured by Cardiac Magnetic Resonance Predicts Cardiovascular Morbidity and Death
Abstract
Background: Myocardial strain using cardiac magnetic resonance (CMR) is a sensitive marker for predicting adverse outcomes in many cardiac disease states, but the prognostic value in the general population has not been studied conclusively.
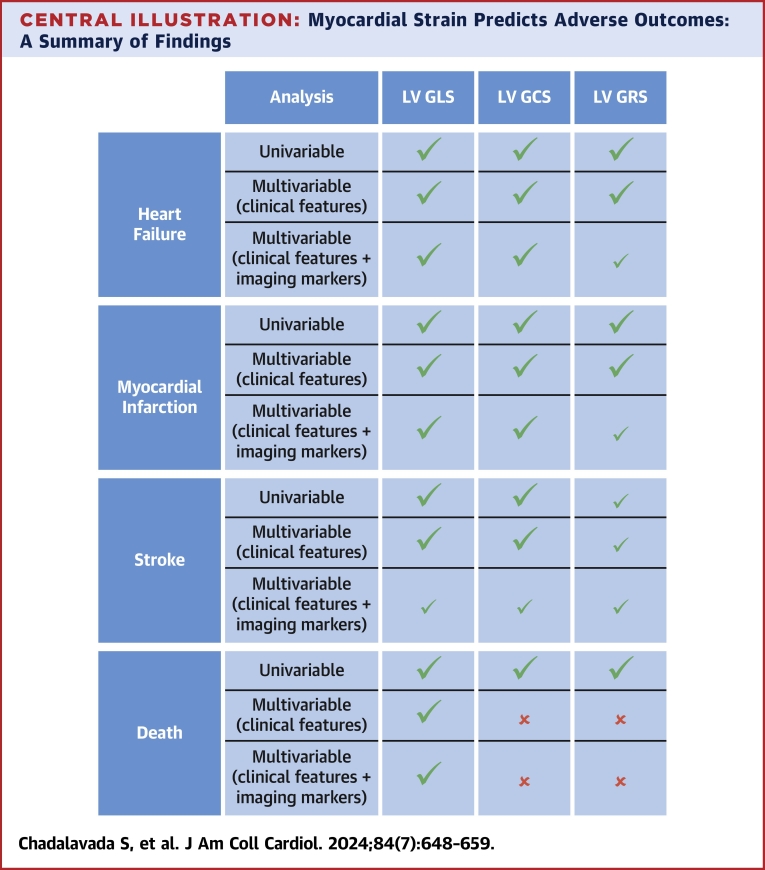
Objectives: The goal of this study was to assess the independent prognostic value of CMR feature tracking (FT)-derived LV global longitudinal (GLS), circumferential (GCS), and radial strain (GRS) metrics in predicting adverse outcomes (heart failure, myocardial infarction, stroke, and death).
Methods: Participants from the UK Biobank population imaging study were included. Univariable and multivariable Cox models were used for each outcome and each strain marker (GLS, GCS, GRS) separately. The multivariable models were tested with adjustment for prognostically important clinical features and conventional global LV imaging markers relevant for each outcome.
Results: Overall, 45,700 participants were included in the study (average age 65 ± 8 years), with a median follow-up period of 3 years. All univariable and multivariable models demonstrated that lower absolute GLS, GCS, and GRS were associated with increased incidence of heart failure, myocardial infarction, stroke, and death. All strain markers were independent predictors (incrementally above some respective conventional LV imaging markers) for the morbidity outcomes, but only GLS predicted death independently: (HR: 1.18; 95% CI: 1.07-1.30).
Conclusions: In the general population, LV strain metrics derived using CMR-FT in radial, circumferential, and longitudinal directions are strongly and independently predictive of heart failure, myocardial infarction, and stroke, but only GLS is independently predictive of death in an adult population cohort.
Keywords: cardiac magnetic resonance; circumferential strain; longitudinal strain; radial strain; survival analysis.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work acknowledges the support of the National Institute for Health and Care Research Barts Biomedical Research Centre (NIHR203330); a delivery partnership of Barts Health NHS Trust, Queen Mary University of London, St George’s University Hospitals NHS Foundation Trust and St George’s University of London. Barts Charity (G-002346) contributed to fees required to access UK Biobank data [access application #2964]. This paper is supported by the London Medical Imaging and Artificial Intelligence Centre for Value Based Healthcare (AI4VBH), which is funded from the Data to Early Diagnosis and Precision Medicine strand of the government’s Industrial Strategy Challenge Fund, managed and delivered by Innovate UK on behalf of UK Research and Innovation (UKRI). Views expressed are those of the authors and not necessarily those of the AI4VBH Consortium members, the NHS, Innovate UK, or UKRI. The funders did not have any role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. Dr Petersen acknowledges the British Heart Foundation for funding the manual analysis to create a cardiovascular magnetic resonance imaging reference standard for the UK Biobank imaging resource in 5,000 CMR scans (PG/14/89/31194). Dr Aung acknowledges the Medical Research Council for supporting his Clinician Scientist Fellowship (MR/X020924/1). Dr Chadalavada was funded by European Union's Horizon 2020 research and innovation program under grant agreement no. 825903 (euCanSHare project). Dr Rauseo is supported by the mini-Centre for Doctoral Training (CDT) award through the Faculty of Science and Engineering, Queen Mary University of London, United Kingdom. Dr Naderi was supported by the British Heart Foundation Pat Merriman Clinical Research Training Fellowship (FS/20/22/34640). Dr Petersen and Dr Lee acknowledge support from the SmartHeart EPSRC program grant (EP/P001009/1) and the European Union's Horizon 2020 research and innovation program under grant agreement No 825903 (euCanSHare project). Dr Petersen has served as a consultant for Cardiovascular Imaging Inc, Calgary, Alberta, Canada. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- Marwick T.H. Ejection fraction pros and cons: JACC state-of-the-art review. J Am Coll Cardiol. 2018;72:2360–2379. - PubMed
-
- Mangion K., McComb C., Auger D.A., Epstein F.H., Berry C. Magnetic resonance imaging of myocardial strain after acute ST-segment-elevation myocardial infarction a systematic review. Circ Cardiovasc Imaging. 2017;10 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
