

Identification of genetic subtypes in follicular lymphoma
- PMID: 39112453
- PMCID: PMC11306633
- DOI: 10.1038/s41408-024-01111-w
Identification of genetic subtypes in follicular lymphoma
Abstract
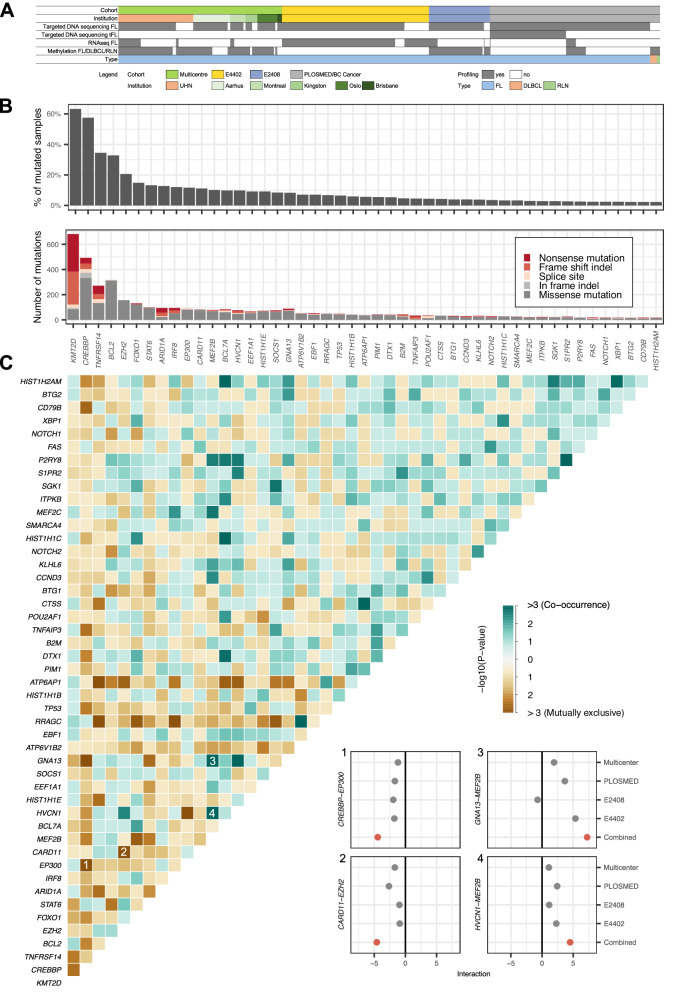
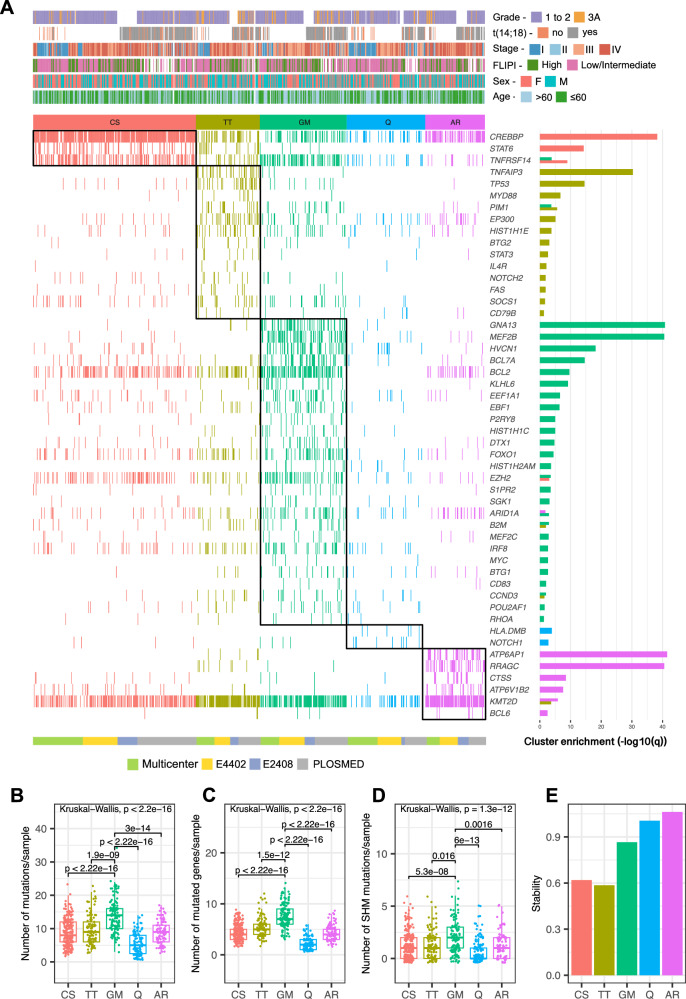
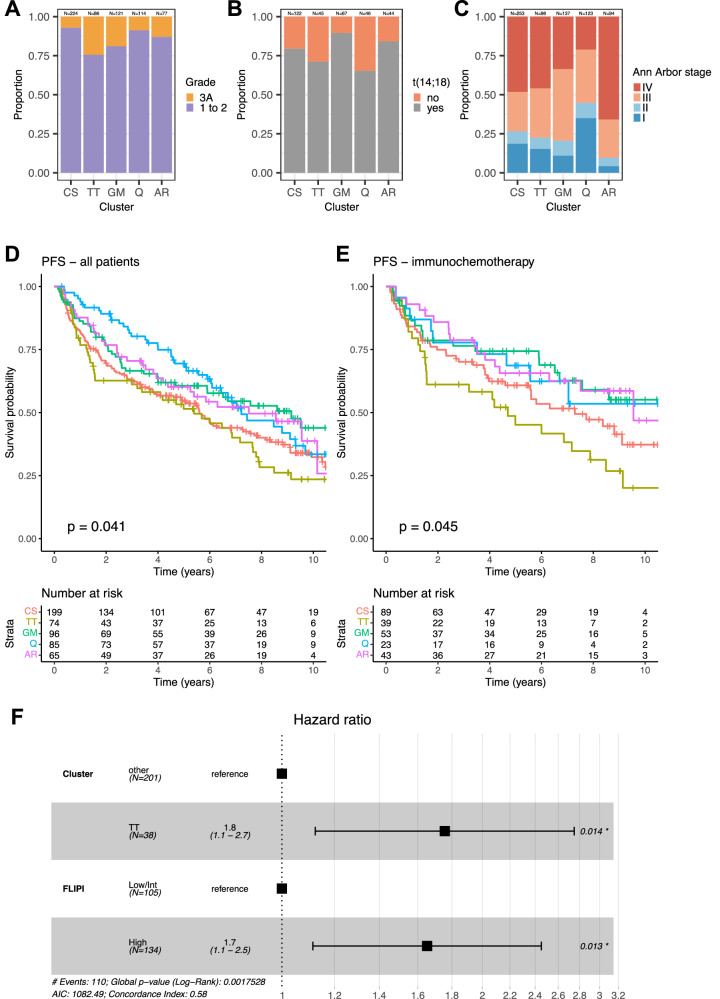
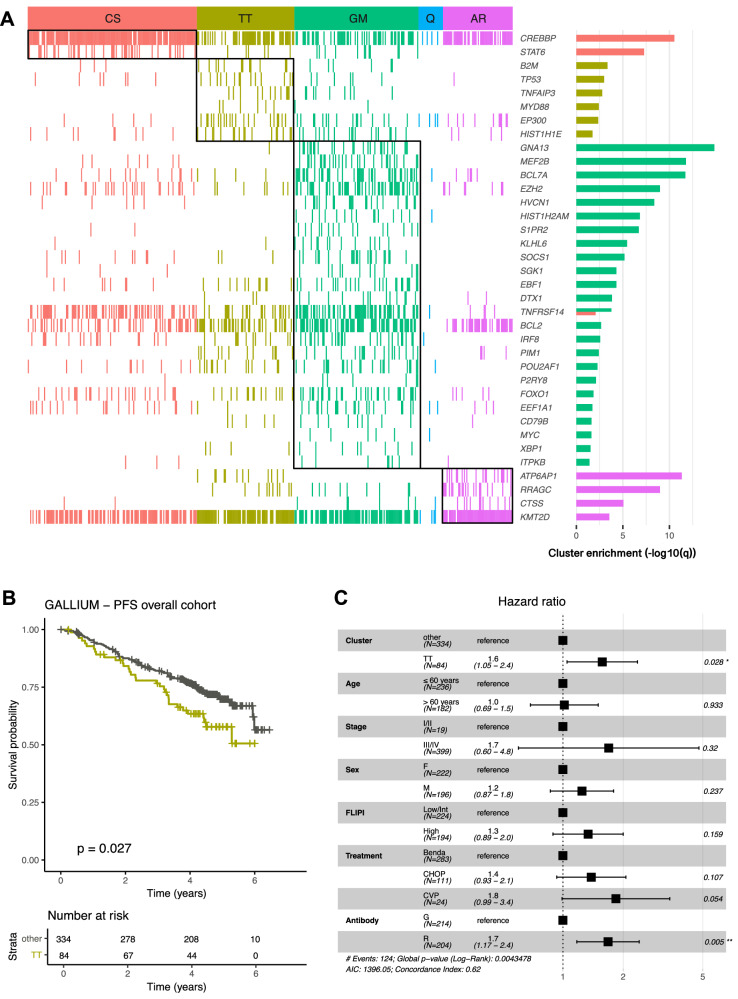
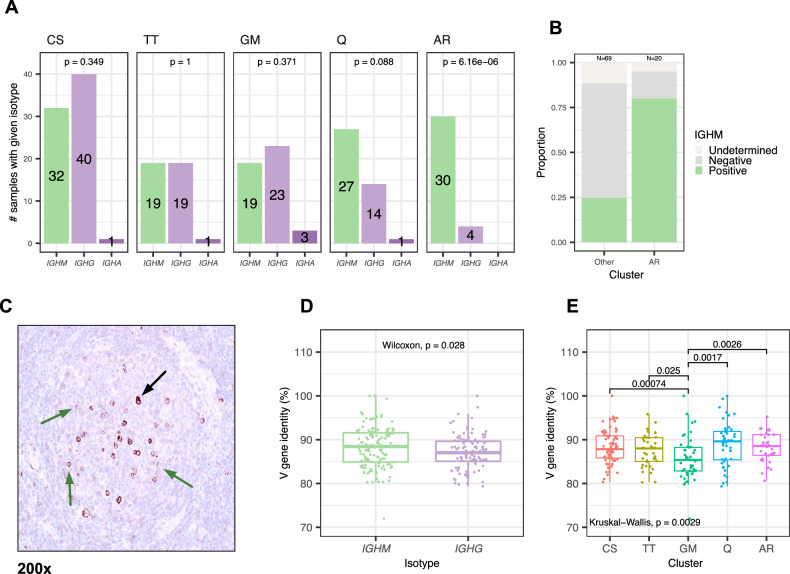
Follicular lymphoma (FL) exhibits considerable variability in biological features and clinical trajectories across patients. To dissect the diversity of FL, we utilized a Bernoulli mixture model to identify genetic subtypes in 713 pre-treatment tumor tissue samples. Our analysis revealed the existence of five subtypes with unique genetic profiles that correlated with clinicopathological characteristics. The clusters were enriched in specific mutations as follows: CS (CREBBP and STAT6), TT (TNFAIP3 and TP53), GM (GNA13 and MEF2B), Q (quiescent, for low mutation burden), and AR (mutations of mTOR pathway-related genes). The subtype Q was enriched for patients with stage I disease and associated with a lower proliferative history than the other subtypes. The AR subtype was unique in its enrichment for IgM-expressing FL cases and was associated with advanced-stage and more than 4 nodal sites. The existence of subtypes was validated in an independent cohort of 418 samples from the GALLIUM trial. Notably, patients assigned to the TT subtype consistently experienced inferior progression-free survival when treated with immunochemotherapy. Our findings offer insight into core pathways distinctly linked with each FL cluster and are expected to be informative in the era of targeted therapies.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Casulo C, Byrtek M, Dawson KL, Zhou X, Farber CM, Flowers CR, et al. Early relapse of follicular lymphoma after rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone defines patients at high risk for death: an analysis from the National LymphoCare Study. J Clin Oncol. 2015;33:2516–22. 10.1200/JCO.2014.59.7534 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 513421/Leukemia and Lymphoma Society of Canada (Leukemia & Lymphoma Society of Canada)
- U24 CA196172/CA/NCI NIH HHS/United States
- 6599-20/Leukemia and Lymphoma Society (Leukemia & Lymphoma Society)
- 2021_EKES.13/Else Kröner-Fresenius-Stiftung (Else Kroner-Fresenius Foundation)
- U10 CA180820/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
