

Assessing the impact of COVID-19 management on the workload of human resources working in India's National Tuberculosis Elimination Program
- PMID: 39113002
- PMCID: PMC11308665
- DOI: 10.1186/s12913-024-11131-8
Assessing the impact of COVID-19 management on the workload of human resources working in India's National Tuberculosis Elimination Program
Abstract
Background: In 1993, WHO declared tuberculosis (TB) as a global health emergency considering 10 million people are battling TB, of which 30% are undiagnosed annually. In 2020 the COVID-19 pandemic took an unprecedented toll on health systems in every country. Public health staff already engaged in TB control and numerous other departments were additionally tasked with managing COVID-19, stretching human resource (HR) capacity beyond its limits. As part of an assessment of HR involved in TB control in India, The World Bank Group and partners conducted an analysis of the impact of COVID-19 on TB human resources for health (HRH) workloads, with the objective of describing the extent to which TB-related activities could be fulfilled and hypothesizing on future HR requirements to meet those needs.
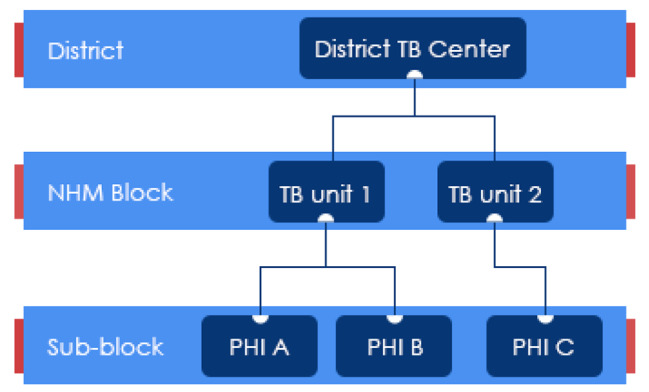
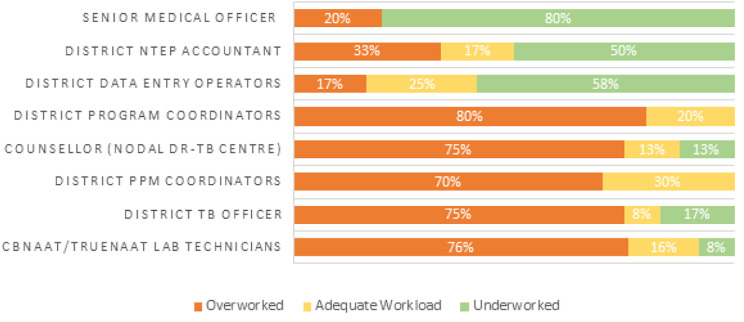
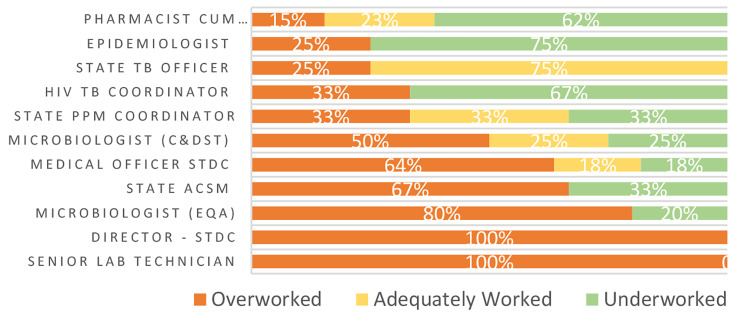
Methods: The study team conducted a Workload Indicators and Staffing Needs (WISN) analysis according to standard WHO methodology to classify the workloads of priority cadres directly or indirectly involved in TB control activities as over-, adequately or under-worked, in 18 districts across seven states in India. Data collection was done via telephone interviews, and questions were added regarding the proportion of time dedicated to COVID-19 related tasks. We carried out quantitative analysis to describe the time allocated to COVID-19 which otherwise would have been spent on TB activities. We also conducted key informant interviews (KII) with key TB program staff about HRH planning and task-shifting from TB to COVID-19.
Results: Workload data were collected from 377 respondents working in or together with India's Central TB Division (CTD). 73% of all respondents (n = 270) reported carrying out COVID-19 tasks. The average time spent on COVID-19 tasks was 4 h / day (n = 72 respondents). Multiple cadres highly instrumental in TB screening and diagnosis, in particular community outreach (ASHA) workers and CBNAAT/TrueNAAT laboratory technicians working at peripheral, block and district levels, were overworked, and spending more than 50% of their time on COVID-19 tasks, reducing time for TB case-finding. Qualitative interviews with laboratory technicians revealed that PCR machines previously used for TB testing were repurposed for COVID-19 testing.
Conclusions: The devastating impact of COVID-19 on HR capacity to conduct TB case-finding in India, as in other settings, cannot be overstated. Our findings provide clear evidence that NTEP human resources did not have time or essential material resources to carry out TB tasks during the COVID pandemic without doing substantial overtime and/or compromising on TB service delivery. To minimize disruptions to routine health services such as TB amidst future emerging infectious diseases, we would do well, during periods of relative calm and stability, to strategically map out how HRH lab staff, public health resources, such as India's Health and Wellness Centers and public health cadre, and public-private sector collaboration can most optimally absorb shocks to the health system.
Keywords: COVID-19; Human resources for health; Tuberculosis.
© 2024. The Author(s).
Conflict of interest statement
We have no competing interests to declare.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
