

Association between triglyceride-glucose related indices and all-cause and cause-specific mortality in the general population: a cohort study
- PMID: 39113049
- PMCID: PMC11304911
- DOI: 10.1186/s12933-024-02390-0
Association between triglyceride-glucose related indices and all-cause and cause-specific mortality in the general population: a cohort study
Abstract
Background: Although triglyceride-glucose (TyG) index is a reliable indicator of insulin resistance and cardiometabolic disease, its effectiveness in predicting mortality risk has not been adequately validated. We aimed to investigate the association between the TyG-related indices and all-cause and cause-specific mortality in the general population.
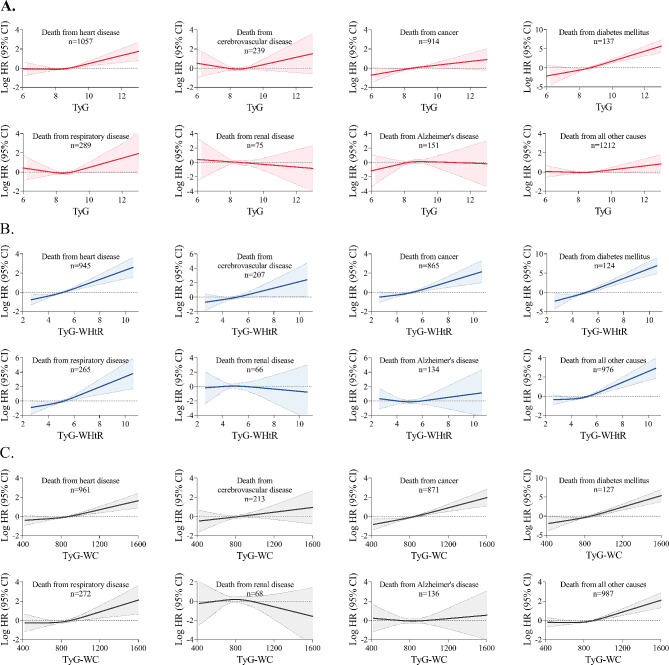
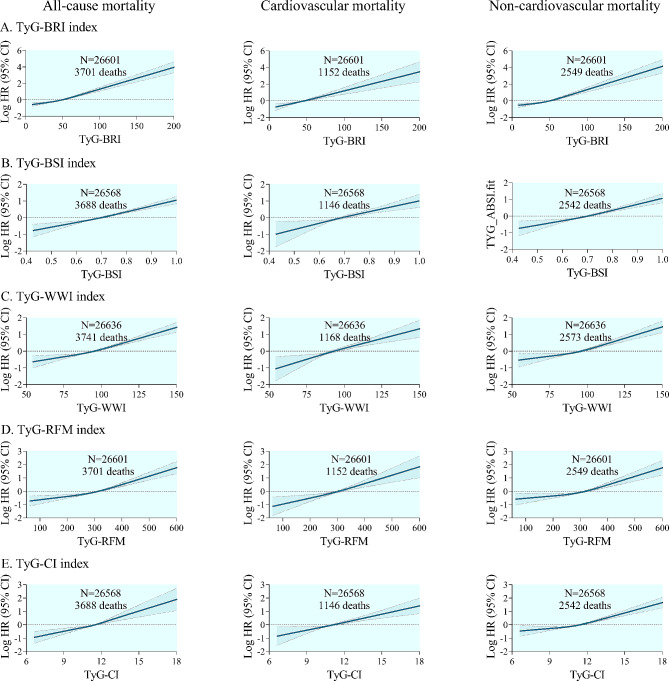
Methods: A total of 27,642 individuals were included from the National Health and Nutrition Examination Survey (NHANES) between 1999 and 2018. Three indicators were constructed, including the TyG index, TyG combined with waist-to-height ratio (TyG-WHtR), and TyG combined with waist circumference (TyG-WC). Mortality data was acquired through the linkage of NHANES data with National Death Index records. Weighted Cox proportional hazards models were used to estimate the independent association between the TyG-related indices and mortality. Nonlinear associations were explored using restricted cubic splines.
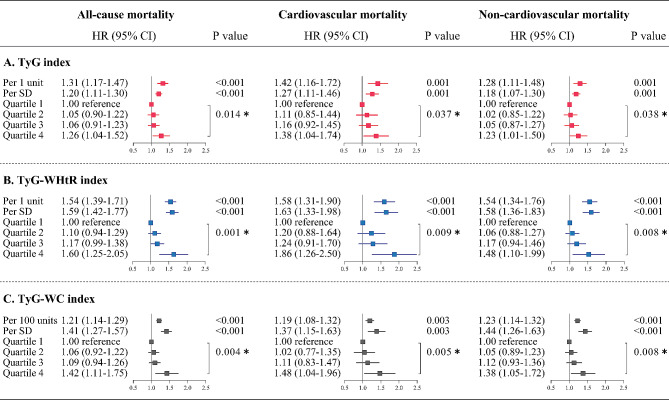
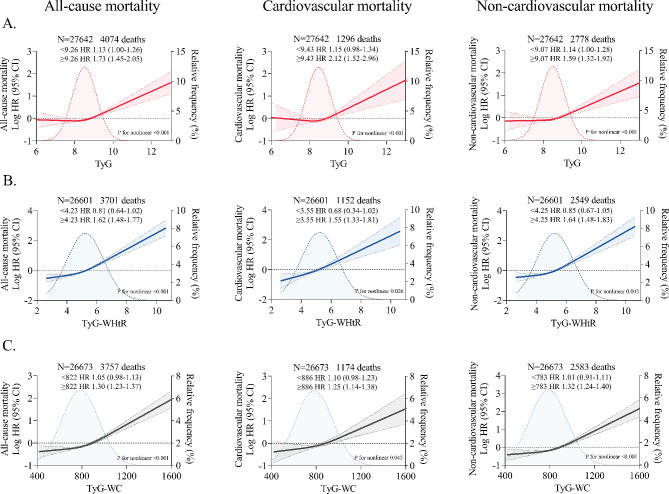
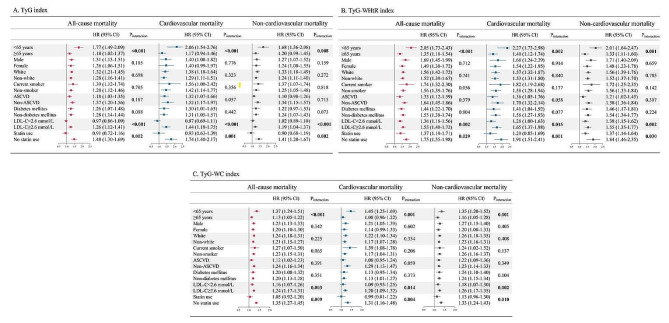
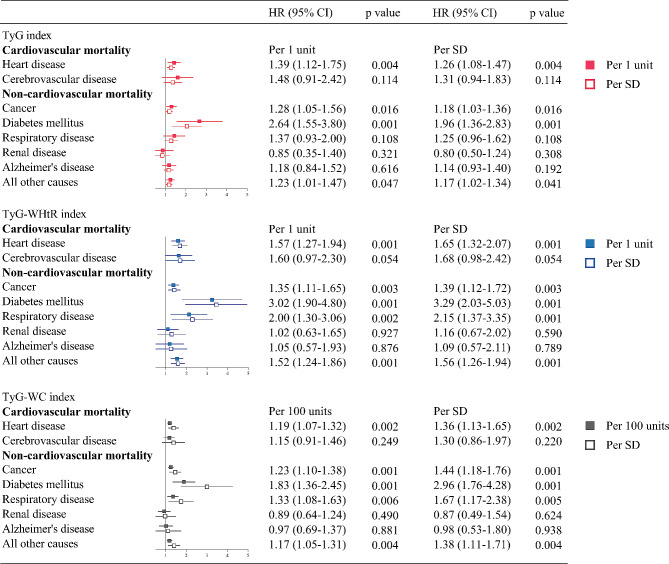
Results: Multivariable adjusted models showed a progressive increase in all-cause and cause-specific mortality across quartiles of the TyG-related indices. Compared with the lowest quartile of the TyG index, the highest quartile had adjusted hazard ratios of 1.26 (95% CI 1.04-1.52) for all-cause mortality, 1.38 (1.04-1.74) for cardiovascular mortality, and 1.23 (1.01-1.50) for non-cardiovascular mortality, respectively. For the TyG-WHtR index, the corresponding hazard ratios were 1.60 (1.25-2.05), 1.86 (1.26-2.50), and 1.48 (1.10-1.99), respectively. For the TyG-WC index, the corresponding hazard ratios were 1.42 (1.11-1.75), 1.48 (1.04-1.96), and 1.38 (1.05-1.72), respectively. The associations between the three TyG-related indices and all-cause, cardiovascular and non-cardiovascular mortality were J-shaped. Interaction tests revealed significant effect modification by age, low-density lipoprotein cholesterol (LDL-C) level, and statin use (all P values < 0.05).
Conclusions: The TyG-related indices were independent predictors of all-cause and cause-specific mortality in the general population. Young individuals should be particularly vigilant, whereas low LDL-C levels and statin use are potentially protective.
Keywords: All-cause mortality; Anthropometric measure; Cause-specific mortality; Triglyceride-glucose index; Waist circumference; Waist-to-height ratio.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World health statistics. 2024: monitoring health for the SDGs, sustainable development goals. [https://www.who.int/data/gho/publications/world-health-statistics. Accessed 21 May 2024.].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
