

Obesity and 1-year all-cause survival of adult intensive care patients with heart failure: data from the MIMIC-IV
- PMID: 39113062
- PMCID: PMC11304645
- DOI: 10.1186/s13098-024-01428-3
Obesity and 1-year all-cause survival of adult intensive care patients with heart failure: data from the MIMIC-IV
Abstract
Background: Heart failure is a disease that threatens global public safety. In recent years, the obesity paradox has been studied in cardiovascular disease and other fields. With the progress of aging, metabolic changes and regulation of fat function, it also provides many bridges for the dialogue between disease and molecular metabolism. The purpose of this study is to investigate the effect of obesity on the outcome of adult intensive care patients with heart failure combined with age factors.
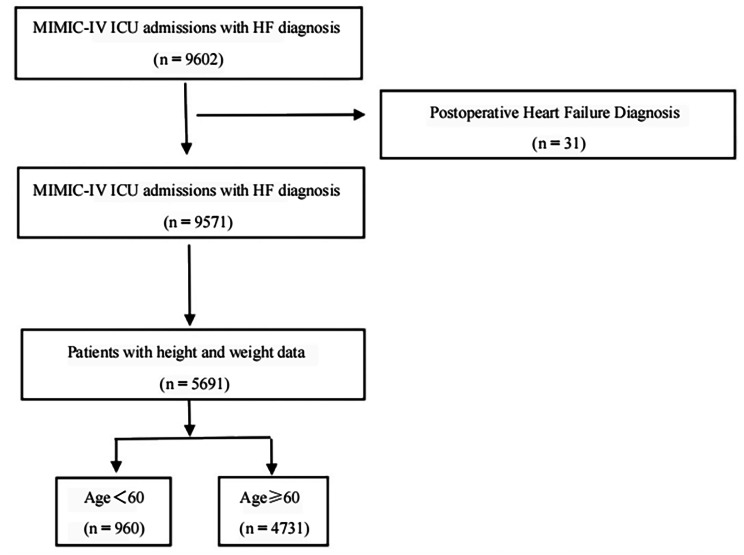
Method: Data were derived from the fourth-generation Medical Information Marketplace for Intensive Care (MIMIC-IV version2.1) using structured query language on the Navicat (12.0.11) platform. People were divided into two groups based on the body mass index (BMI), one group with BMI ≥ 30 kg/m² and another group with BMI < 30 kg/m². Afterwards, the patients were divided into two subgroups based on their ages. One group included patients aged<60, and the other included patients aged ≥ 60. The extracted information includes demographic characteristics, laboratory findings, comorbidities, scores. Main results included in-hospital mortality, ICU mortality, and 1-year mortality. Secondary outcomes included hospital interval and ICU interval, use of renal replacement therapy, and rates of noninvasive and invasive ventilation support.
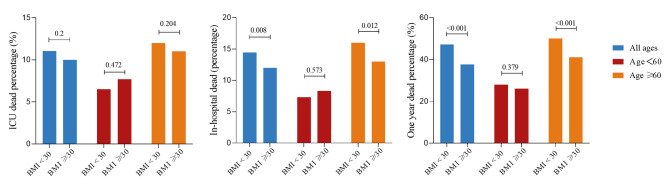
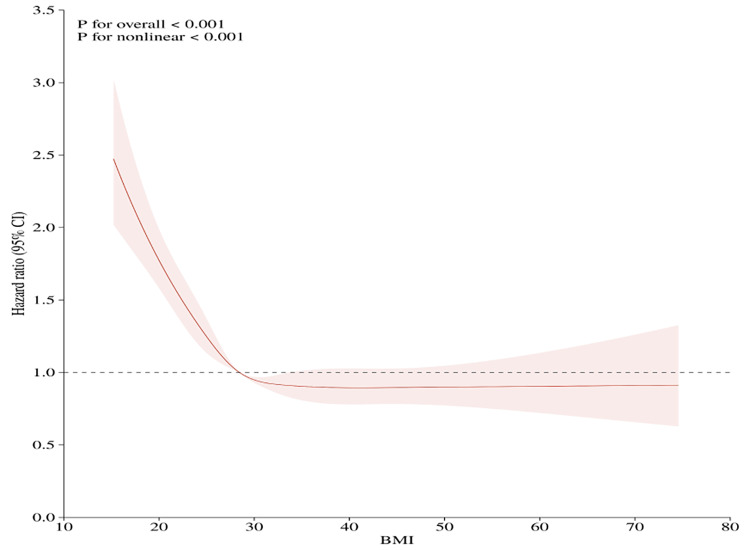
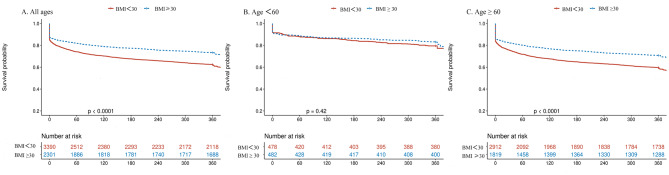
Result: In this cohort study, 3390 people were in the BMI<30 group, 2301 people were in the BMI ≥ 30 group, 960 people were in the age<60 group, and 4731 people were in the age ≥ 60 group, including 3557 patients after propensity score matching in high age group. Among patients aged ≥ 60, BMI ≥ 30 group vs. BMI<30 group showed significantly lower in-hospital mortality (13% vs. 16%) and one-year mortality (41% vs. 55%), respectively. Neither primary nor secondary outcomes were significantly described in the competition among patients aged under 60. Restricted cubic spline reveals a J-shaped nonlinear association between BMI and clinical endpoints within the entire cohort. Kaplan-Meier curves revealed a survival advantage in BMI ≥ 30 group (p < 0.001). Following age stratification, a beneficial effect of BMI categories on one-year mortality risk was observed in heart failure patients aged ≥ 60 (Univariable HR, 0.71, 95% CI, 0.65-0.78, p < 0.001; Multivariable HR, 0.74, 95% CI, 0.67-0.81, p < 0.001), but not in those under 60 years old.
Outcome: In ICU patients with heart failure, obesity offers a survival benefit to those aged ≥ 60. No obesity paradox was observed in patients younger than 60 years old. The obesity paradox applies to patients aged ≥ 60 with heart failure.
Keywords: Age; BMI; Heart failure; ICU; Survival benefits.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The obesity paradox in younger adult patients with sepsis: analysis of the MIMIC-IV database.Int J Obes (Lond). 2024 Sep;48(9):1223-1230. doi: 10.1038/s41366-024-01523-5. Epub 2024 Apr 26. Int J Obes (Lond). 2024. PMID: 38671071
-
Association between triglyceride glucose-body mass and one-year all-cause mortality of patients with heart failure: a retrospective study utilizing the MIMIC-IV database.Cardiovasc Diabetol. 2023 Nov 8;22(1):309. doi: 10.1186/s12933-023-02047-4. Cardiovasc Diabetol. 2023. PMID: 37940979 Free PMC article.
-
Impact of the obesity paradox on 28-day mortality in elderly patients critically ill with cardiogenic shock: a retrospective cohort study.Diabetol Metab Syndr. 2024 Dec 3;16(1):292. doi: 10.1186/s13098-024-01538-y. Diabetol Metab Syndr. 2024. PMID: 39623391 Free PMC article.
-
Is body mass index associated with outcomes of mechanically ventilated adult patients in intensive critical units? A systematic review and meta-analysis.PLoS One. 2018 Jun 8;13(6):e0198669. doi: 10.1371/journal.pone.0198669. eCollection 2018. PLoS One. 2018. PMID: 29883469 Free PMC article.
-
Body mass index and all-cause mortality in heart failure patients with normal and reduced ventricular ejection fraction: a dose-response meta-analysis.Clin Res Cardiol. 2019 Feb;108(2):119-132. doi: 10.1007/s00392-018-1302-7. Epub 2018 Jun 27. Clin Res Cardiol. 2019. PMID: 29951802 Review.
Cited by
-
The association between obesity indicators and mortality among individuals with hyperlipidemia: evidence from the NHANES 2003-2018.Lipids Health Dis. 2025 Jan 24;24(1):20. doi: 10.1186/s12944-025-02442-8. Lipids Health Dis. 2025. PMID: 39856680 Free PMC article.
-
Association between body mass index and long-term all-cause mortality in critically ill patients without malignant tumors.PLoS One. 2025 Jun 25;20(6):e0325452. doi: 10.1371/journal.pone.0325452. eCollection 2025. PLoS One. 2025. PMID: 40560851 Free PMC article.
References
-
- Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N, Anker SD, Atherton J, Böhm M, Butler J, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart failure: endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese heart failure Association. Eur J Heart Fail. 2021;23(3):352–80. 10.1002/ejhf.2115 - DOI - PubMed
LinkOut - more resources
Full Text Sources
