

Effect of rosuvastatin versus atorvastatin on new-onset diabetes mellitus in patients treated with high-intensity statin therapy for coronary artery disease: a post-hoc analysis from the LODESTAR randomized clinical trial
- PMID: 39113067
- PMCID: PMC11304915
- DOI: 10.1186/s12933-024-02386-w
Effect of rosuvastatin versus atorvastatin on new-onset diabetes mellitus in patients treated with high-intensity statin therapy for coronary artery disease: a post-hoc analysis from the LODESTAR randomized clinical trial
Abstract
Background: The impact of rosuvastatin versus atorvastatin on new-onset diabetes mellitus (NODM) among patients treated with high-intensity statin therapy for coronary artery disease (CAD) remains to be clarified. This study aimed to evaluate the risk of NODM in patients with CAD treated with rosuvastatin compared to atorvastatin in the randomized LODESTAR trial.
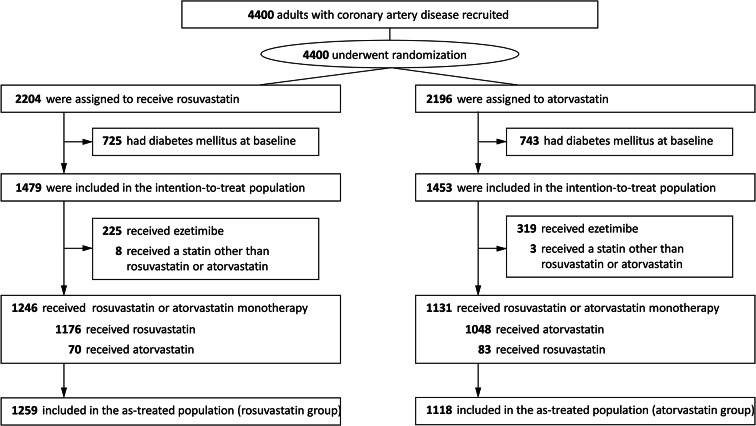
Methods: In the LODESTAR trial, patients with CAD were randomly assigned to receive either rosuvastatin or atorvastatin using a 2-by-2 factorial randomization. In this post-hoc analysis, the 3-year incidence of NODM was compared between rosuvastatin and atorvastatin treatment in the as-treated population with high-intensity statin therapy as the principal population of interest.
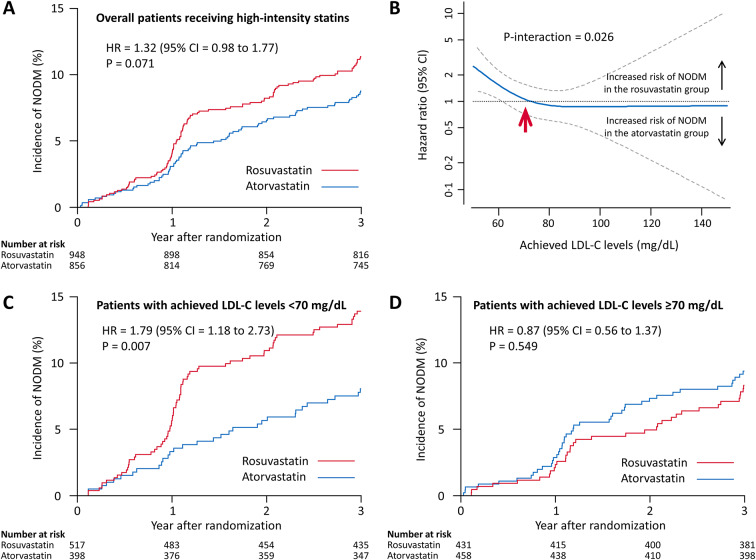
Results: Among 2932 patients without diabetes mellitus at baseline, 2377 were included in the as-treated population analysis. In the as-treated population with high-intensity statin therapy, the incidence of NODM was not significantly different between the rosuvastatin and atorvastatin groups (11.4% [106/948] versus 8.8% [73/856], hazard ratio [HR] = 1.32, 95% confidence interval [CI] = 0.98 to 1.77, P = 0.071). When the risk of NODM with rosuvastatin versus atorvastatin was assessed according to the achieved low-density lipoprotein cholesterol (LDL-C) level, the risk of NODM began to increase at a LDL-C level below 70 mg/dL. The incidence of NODM was significantly greater in the rosuvastatin group than it was in the atorvastatin group when the achieved LDL-C level was < 70 mg/dL (13.9% versus 8.0%; HR = 1.79, 95% CI 1.18 to 2.73, P = 0.007).
Conclusions: Among CAD patients receiving high-intensity statin therapy, the incidence of NODM was not significantly different between rosuvastatin and atorvastatin. However, a drug effect of the statin type on NODM was observed when the achieved LDL-C level was < 70 mg/dL.
Trial registration: ClinicalTrials.gov, Identifier: NCT02579499.
Keywords: Coronary artery disease; Diabetes mellitus; Statin.
© 2024. The Author(s).
Conflict of interest statement
M-KH has received speaker’s fees from Medtronic, Edward Lifesciences, and Viatris Korea and institutional research grants from Sam Jin Pharmaceutical and Chong Kun Dang Pharmaceutical. All other authors declare no competing interests.
Figures
References
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019;139(25):e1082–143. - PMC - PubMed
-
- Mach F, Ray KK, Wiklund O, Corsini A, Catapano AL, Bruckert E, et al. Adverse effects of statin therapy: perception vs. the evidence - focus on glucose homeostasis, cognitive, renal and hepatic function, haemorrhagic stroke and cataract. Eur Heart J. 2018;39(27):2526–39. 10.1093/eurheartj/ehy182 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
