

Cord blood transfusions in extremely low gestational age neonates to reduce severe retinopathy of prematurity: results of a prespecified interim analysis of the randomized BORN trial
- PMID: 39113069
- PMCID: PMC11305044
- DOI: 10.1186/s13052-024-01714-w
Cord blood transfusions in extremely low gestational age neonates to reduce severe retinopathy of prematurity: results of a prespecified interim analysis of the randomized BORN trial
Abstract
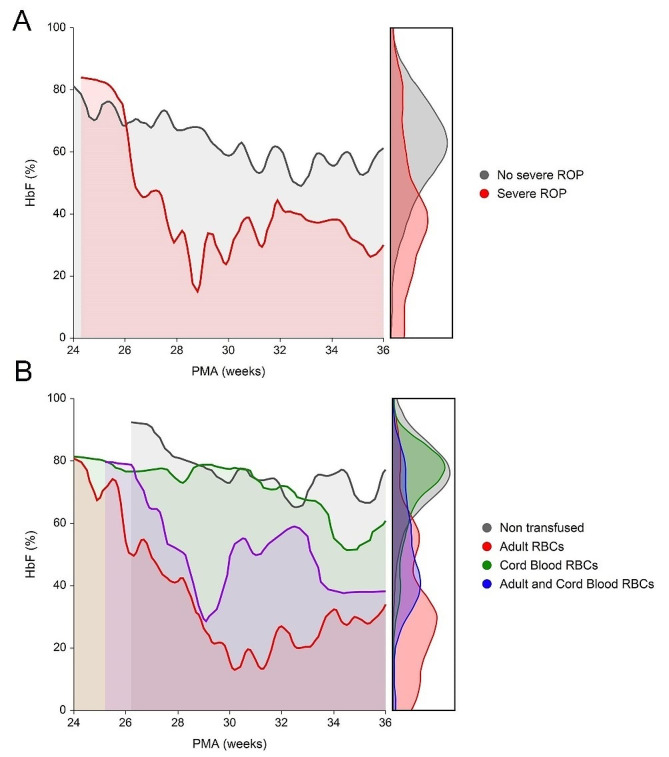
Background: Preterm infants are at high risk for retinopathy of prematurity (ROP), with potential life-long visual impairment. Low fetal hemoglobin (HbF) levels predict ROP. It is unknown if preventing the HbF decrease also reduces ROP.
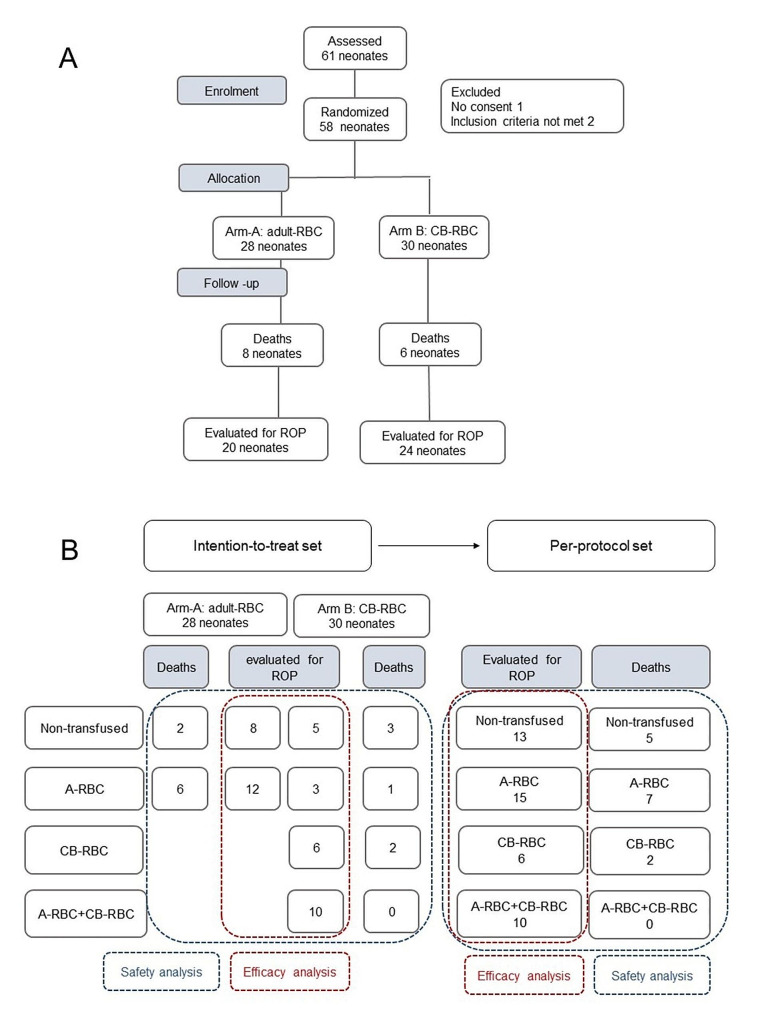
Methods: BORN is an ongoing multicenter double-blinded randomized controlled trial investigating whether transfusing HbF-enriched cord blood-red blood cells (CB-RBCs) instead of adult donor-RBC units (A-RBCs) reduces the incidence of severe ROP (NCT05100212). Neonates born between 24 and 27 + 6 weeks of gestation are enrolled and randomized 1:1 to receive adult donor-RBCs (A-RBCs, arm A) or allogeneic CB-RBCs (arm B) from birth to the postmenstrual age (PMA) of 31 + 6 weeks. Primary outcome is the rate of severe ROP at 40 weeks of PMA or discharge, with a sample size of 146 patients. A prespecified interim analysis was scheduled after the first 58 patients were enrolled, with the main purpose to evaluate the safety of CB-RBC transfusions.
Results: Results in the intention-to-treat and per-protocol analysis are reported. Twenty-eight patients were in arm A and 30 in arm B. Overall, 104 A-RBC units and 49 CB-RBC units were transfused, with a high rate of protocol deviations. A total of 336 adverse events were recorded, with similar incidence and severity in the two arms. By per-protocol analysis, patients receiving A-RBCs or both RBC types experienced more adverse events than non-transfused patients or those transfused exclusively with CB-RBCs, and suffered from more severe forms of bradycardia, pulmonary hypertension, and hemodynamically significant patent ductus arteriosus. Serum potassium, lactate, and pH were similar after CB-RBCs or A-RBCs. Fourteen patients died and 44 were evaluated for ROP. Ten of them developed severe ROP, with no differences between arms. At per-protocol analysis each A-RBC transfusion carried a relative risk for severe ROP of 1.66 (95% CI 1.06-2.20) in comparison with CB-RBCs. The area under the curve of HbF suggested that HbF decrement before 30 weeks PMA is critical for severe ROP development. Subsequent CB-RBC transfusions do not lessen the ROP risk.
Conclusions: The interim analysis shows that CB-RBC transfusion strategy in preterm neonates is safe and, if early adopted, might protect them from severe ROP.
Trial registration: Prospectively registered at ClinicalTrials.gov on October 29, 2021. Identifier number NCT05100212.
Keywords: ELGAN; HbF; ROP; Randomized controlled trial; Transfusions; Umbilical blood.
© 2024. The Author(s).
Conflict of interest statement
Carlo Dani is a member of the editorial board of Italian Journal of Pediatrics. The authors report no potential conflicts of interest, including relevant financial interests, activities, relationships, and affiliations.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
