

Carbapenem-resistant Enterobacterales sepsis following endoscopic retrograde cholangiopancreatography: risk factors for 30-day all-cause mortality and the development of a nomogram based on a retrospective cohort
- PMID: 39113089
- PMCID: PMC11304701
- DOI: 10.1186/s13756-024-01441-1
Carbapenem-resistant Enterobacterales sepsis following endoscopic retrograde cholangiopancreatography: risk factors for 30-day all-cause mortality and the development of a nomogram based on a retrospective cohort
Abstract
Background: Endoscopic retrograde cholangiopancreatography (ERCP) has become a routine endoscopic procedure that is essential for diagnosing and managing various conditions, including gallstone extraction and the treatment of bile duct and pancreatic tumors. Despite its efficacy, post-ERCP infections - particularly those caused by carbapenem-resistant Enterobacterales (CRE) - present significant risks. These risks highlight the need for accurate predictive models to enhance postprocedural care, reduce the mortality risk associated with post-ERCP CRE sepsis, and improve patient outcomes in the context of increasing antibiotic resistance.
Objective: This study aimed to examine the risk factors for 30-day mortality in patients with CRE sepsis following ERCP and to develop a nomogram for accurately predicting 30-day mortality risk.
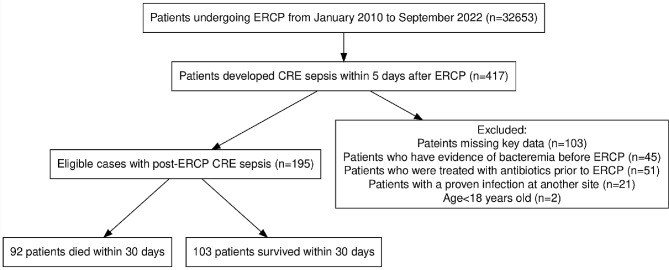
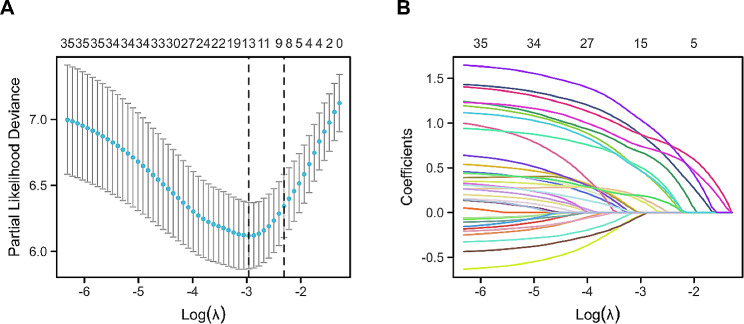
Methods: Data from 195 patients who experienced post-ERCP CRE sepsis between January 2010 and December 2022 were analyzed. Variable selection was optimized via the least absolute shrinkage and selection operator (LASSO) regression model. Multivariate logistic regression analysis was then employed to develop a predictive model, which was evaluated in terms of discrimination, calibration, and clinical utility. Internal validation was achieved through bootstrapping.
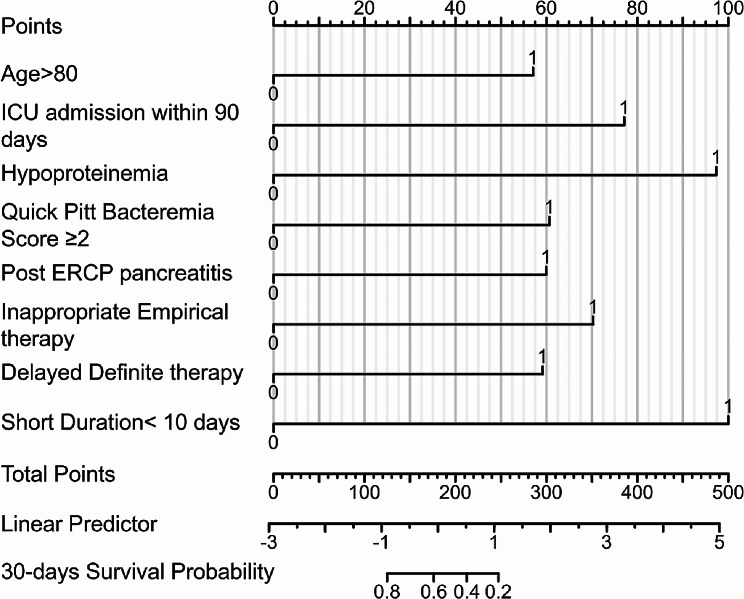
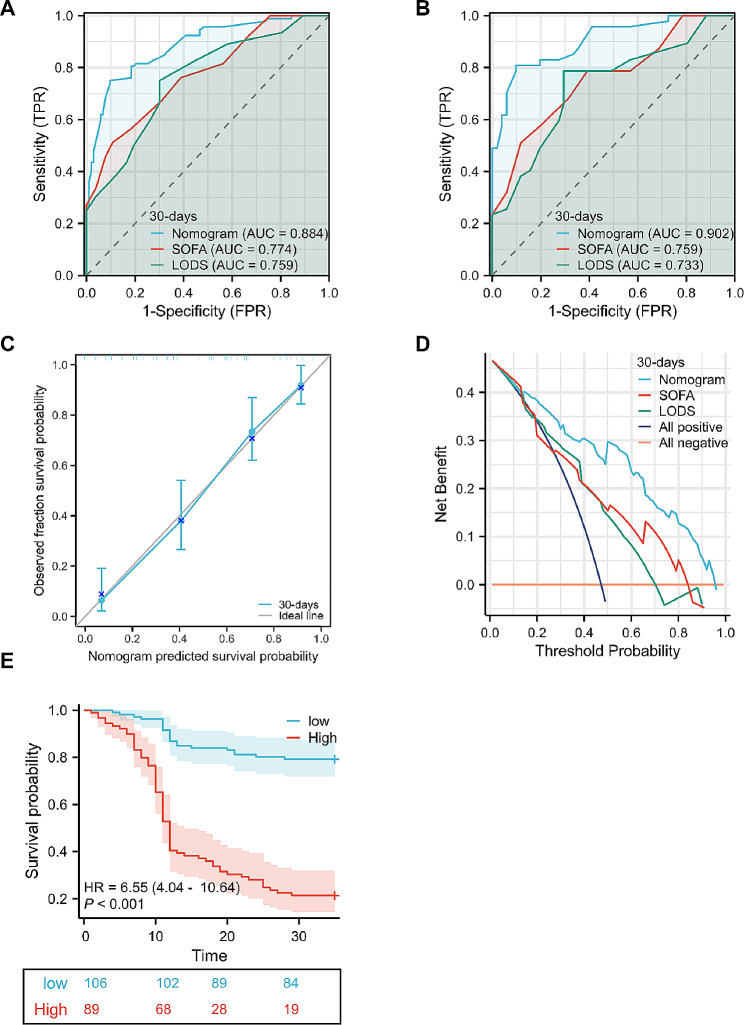
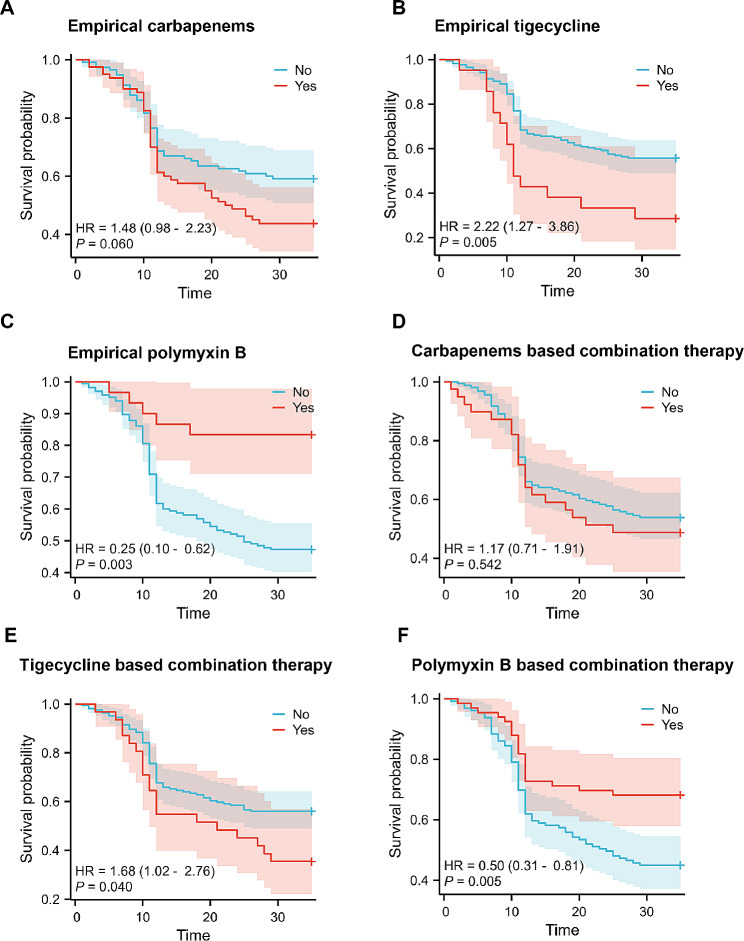
Results: The nomogram included the following predictors: age > 80 years (hazard ratio [HR] 2.61), intensive care unit (ICU) admission within 90 days prior to ERCP (HR 2.64), hypoproteinemia (HR 4.55), quick Pitt bacteremia score ≥ 2 (HR 2.61), post-ERCP pancreatitis (HR 2.52), inappropriate empirical therapy (HR 3.48), delayed definitive therapy (HR 2.64), and short treatment duration (< 10 days) (HR 5.03). The model demonstrated strong discrimination and calibration.
Conclusions: This study identified significant risk factors associated with 30-day mortality in patients with post-ERCP CRE sepsis and developed a nomogram to accurately predict this risk. This tool enables healthcare practitioners to provide personalized risk assessments and promptly administer appropriate therapies against CRE, thereby reducing mortality rates.
Keywords: Carbapenem-resistant Enterobacterales; Endoscopic retrograde cholangiopancreatography; Mortality; Nomogram; Sepsis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Du M, Suo J, Liu B, Xing Y, Chen L, Liu Y. Post-ERCP infection and its epidemiological and clinical characteristics in a large Chinese tertiary hospital: a 4-year surveillance study. Antimicrob Resist Infect Control. 2017;6:131. 10.1186/s13756-017-0290-0. 10.1186/s13756-017-0290-0 - DOI - PMC - PubMed
-
- Hutfless S, Shiratori Y, Chu D, Liu S, Kalloo A. Risk factors for infections after endoscopic retrograde cholangiopancreatography (ERCP): a retrospective cohort analysis of US Medicare Fee-for-Service claims, 2015–2021. BMJ open. 2022;12(9):e065077. 10.1136/bmjopen-2022-065077. 10.1136/bmjopen-2022-065077 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- NSFC No. 82000516/National Natural Science Foundation of China
- 2022ZB271/Zhejiang Chinese Traditional Medicine Scientific Research Fund Project
- A20200737/the Hangzhou Medical and Health Science and Technology Plan
- No. 2024C03048/the Key R&D Program of Zhejiang Province
- No. 2023C03054/the Key R&D Program of Zhejiang Province
LinkOut - more resources
Full Text Sources
Medical
