

Predicting disease recurrence in patients with endometriosis: an observational study
- PMID: 39113136
- PMCID: PMC11304583
- DOI: 10.1186/s12916-024-03508-7
Predicting disease recurrence in patients with endometriosis: an observational study
Abstract
Background: Despite surgical and pharmacological interventions, endometriosis can recur. Reliable information regarding risk of recurrence following a first diagnosis is scant. The aim of this study was to examine clinical and survey data in the setting of disease recurrence to identify predictors of risk of endometriosis recurrence.
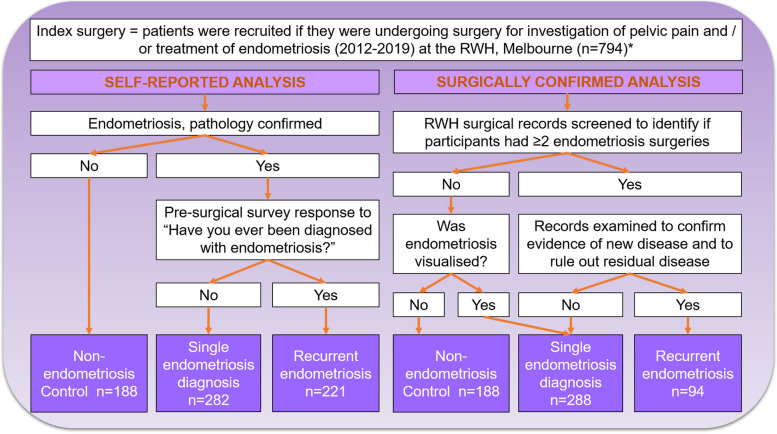
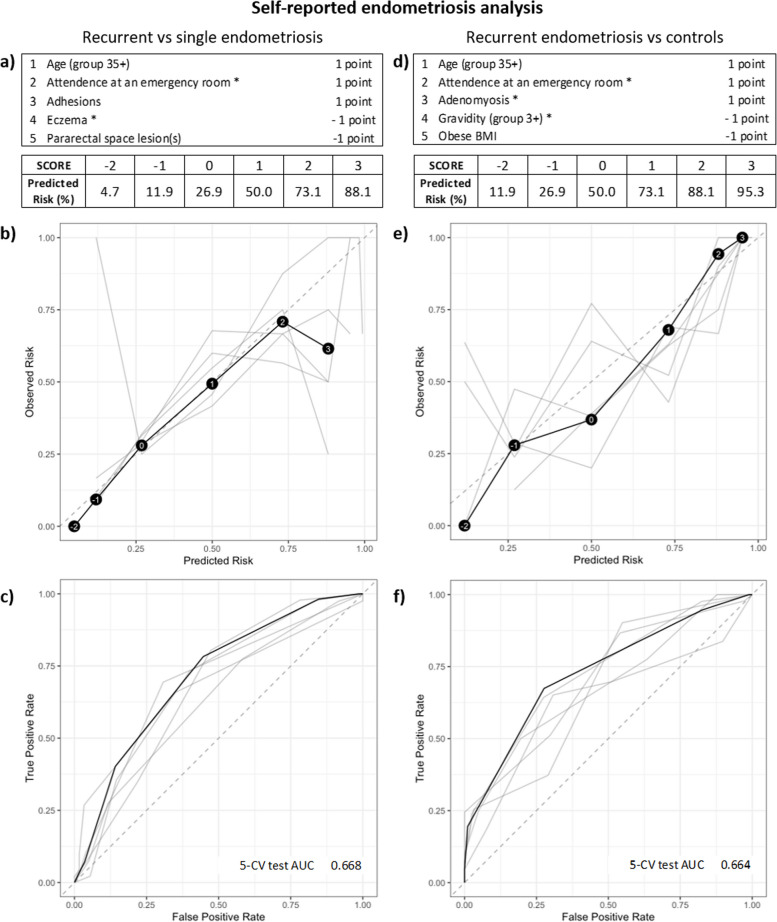
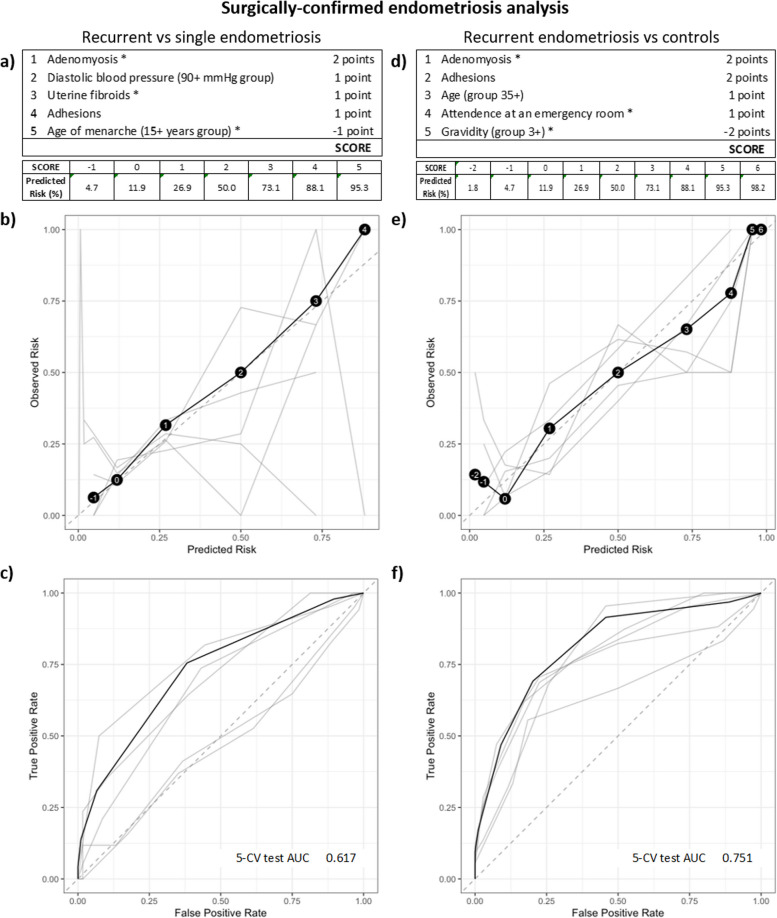
Methods: This observational study reviewed data from 794 patients having surgery for pelvic pain or endometriosis. Patients were stratified into two analytic groups based on self-reported or surgically confirmed recurrent endometriosis. Statistical analyses included univariate, followed by multivariate logistic regression to identify risk factors of recurrence, with least absolute shrinkage and selection operator (Lasso) regularisation. Risk-calibrated Supersparse Linear Integer Models (RiskSLIM) and survival analyses (with Lasso) were undertaken to identify predictive features of recurrence.
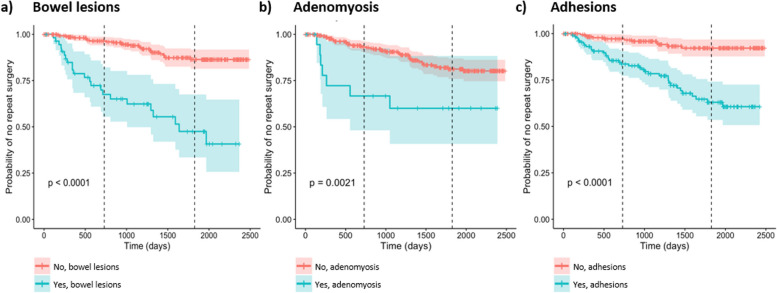
Results: Several significant features were repeatedly identified in association with recurrence, including adhesions, high rASRM score, deep disease, bowel lesions, adenomyosis, emergency room attendance for pelvic pain, younger age at menarche, higher gravidity, high blood pressure and older age. In the surgically confirmed group, with a score of 5, the RiskSLIM method was able to predict the risk of recurrence (compared to a single diagnosis) at 95.3% and included adenomyosis and adhesions in the model. Survival analysis further highlighted bowel lesions, adhesions and adenomyosis.
Conclusions: Following an initial diagnosis of endometriosis, clinical decision-making regarding disease management should take into consideration the presence of bowel lesions, adhesions and adenomyosis, which increase the risk of endometriosis recurrence.
Keywords: Endometriosis; Endometriosis recurrence; Recurrent endometriosis; Reoperation; Repeat surgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
