

The temporal dynamic of bradykinin type 2 receptor effects reveals its neuroprotective role in the chronic phase of cerebral and retinal ischemic injury
- PMID: 39113417
- PMCID: PMC11572167
- DOI: 10.1177/0271678X241270241
The temporal dynamic of bradykinin type 2 receptor effects reveals its neuroprotective role in the chronic phase of cerebral and retinal ischemic injury
Abstract
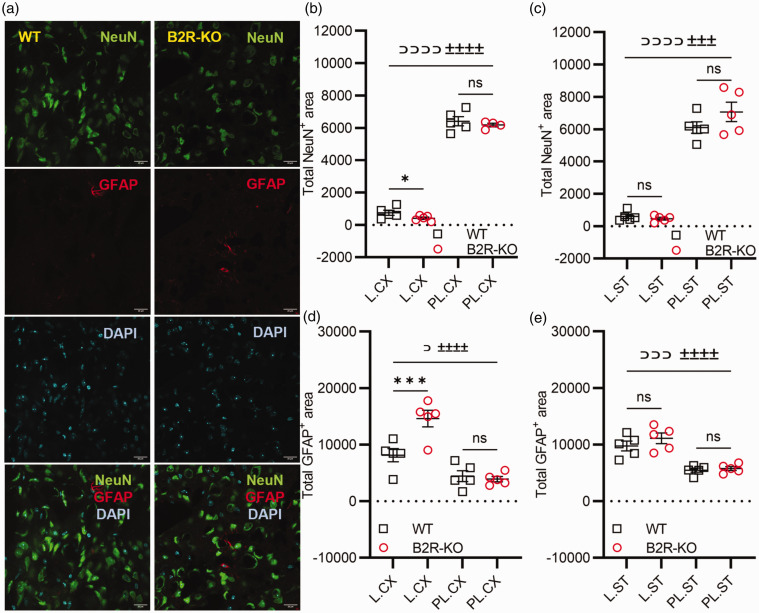
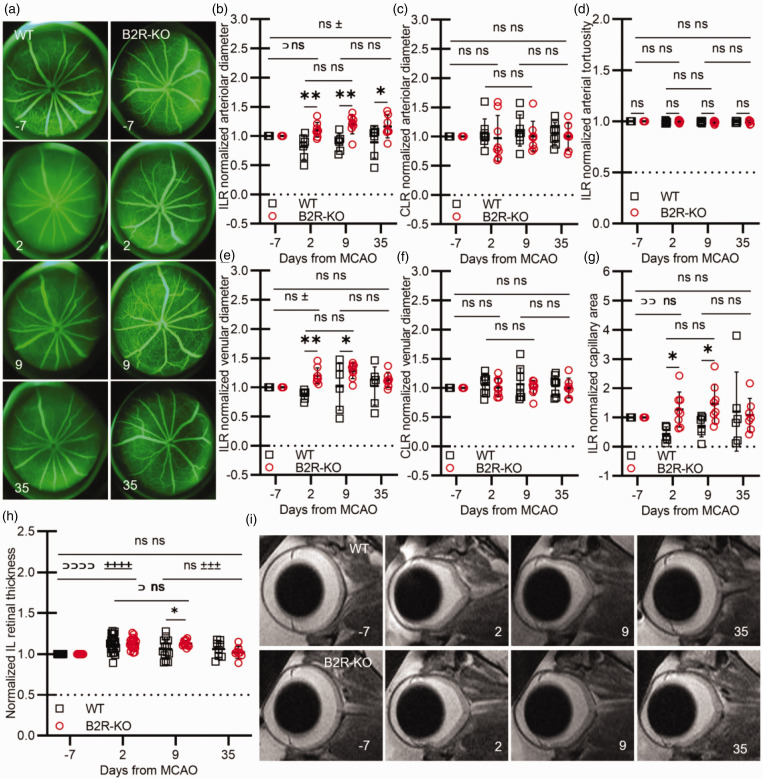
The activation of the bradykinin type 2 receptor is intricately involved in acute post-ischemic inflammatory responses. However, its precise role in different stages of ischemic injury, especially in the chronic phase, remains unclear. Following simultaneous cerebral and retinal ischemia, bradykinin type 2 receptor knockout mice and their controls were longitudinally monitored for 35 days via magnetic resonance imaging, fundus photography, fluorescein angiography, behavioral assessments, vascular permeability measurements, and immunohistochemistry, as well as glycemic status assessments. Without impacting the lesion size, bradykinin type 2 receptor deficiency reduced acute cerebral vascular permeability preventing the loss of pericytes and tight junctions. In the chronic phase of ischemia, however, it resulted in increased astrogliosis and cortical neuronal loss, as well as higher functional deficits. The retinal findings demonstrated a similar pattern. Bradykinin type 2 receptor deficiency delayed, but exacerbated the development of retinal necrosis, increased subacute vascular permeability, and promoted retinal ganglion cell loss in the chronic phase of ischemia. This investigation sheds light on the temporal dynamic of bradykinin type 2 receptor effects in ischemia, pointing to a therapeutic potential in the subacute and chronic phases of ischemic injury.
Keywords: Bradykinin type 2 receptor; brain; ischemia; magnetic resonance imaging; retina.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures





Similar articles
-
Release of bradykinin and expression of kinin B2 receptors in the brain: role for cell death and brain edema formation after focal cerebral ischemia in mice.J Cereb Blood Flow Metab. 2005 Aug;25(8):978-89. doi: 10.1038/sj.jcbfm.9600096. J Cereb Blood Flow Metab. 2005. PMID: 15815587
-
Neuroprotection against retinal ischemia-reperfusion injury by blocking the angiotensin II type 1 receptor.Invest Ophthalmol Vis Sci. 2010 Jul;51(7):3629-38. doi: 10.1167/iovs.09-4107. Epub 2010 Feb 17. Invest Ophthalmol Vis Sci. 2010. PMID: 20164447
-
Blockade of bradykinin receptor B1 but not bradykinin receptor B2 provides protection from cerebral infarction and brain edema.Stroke. 2009 Jan;40(1):285-93. doi: 10.1161/STROKEAHA.108.526673. Epub 2008 Nov 6. Stroke. 2009. PMID: 18988906
-
Involvement of Bradykinin B2 Receptor in Pathological Vascularization in Oxygen-Induced Retinopathy in Mice and Rabbit Cornea.Int J Mol Sci. 2018 Jan 23;19(2):330. doi: 10.3390/ijms19020330. Int J Mol Sci. 2018. PMID: 29360776 Free PMC article.
-
Neuroprotection of bradykinin/bradykinin B2 receptor system in cerebral ischemia.Biomed Pharmacother. 2017 Oct;94:1057-1063. doi: 10.1016/j.biopha.2017.08.042. Epub 2017 Aug 12. Biomed Pharmacother. 2017. PMID: 28810528 Review.
Cited by
-
Thy1-YFP: an effective tool for single cell tracing from neuronal progenitors to mature functionally active neurons.Cell Death Discov. 2025 Jan 22;11(1):18. doi: 10.1038/s41420-025-02297-z. Cell Death Discov. 2025. PMID: 39843432 Free PMC article.
References
-
- Zausinger S, Lumenta D, Pruneau D, et al. Effects of LF 16-0687 Ms, a bradykinin B2 receptor antagonist, on brain edema formation and tissue damage in a rat model of temporary focal cerebral ischemia. Brain Res 2002; 950: 268–278. - PubMed
-
- Walker K, Perkins M, Dray A. Kinins and kinin receptors in the nervous system. Neurochem Int 1995; 26: 1–16. - PubMed
-
- Gröger M, Lebesgue D, Pruneau D, et al. Release of bradykinin and expression of kinin B2 receptors in the brain: Role for cell death and brain edema formation after focal cerebral ischemia in mice. J Cereb Blood Flow Metab 2005; 25: 978–989. - PubMed
-
- Wagner S, Kalb P, Lukosava M, et al. Activation of the tissue kallikrein-kinin system in stroke. J Neurol Sci 2002; 202: 75–76. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
