

GEMA-Na and MELD 3.0 severity scores to address sex disparities for accessing liver transplantation: a nationwide retrospective cohort study
- PMID: 39114271
- PMCID: PMC11304699
- DOI: 10.1016/j.eclinm.2024.102737
GEMA-Na and MELD 3.0 severity scores to address sex disparities for accessing liver transplantation: a nationwide retrospective cohort study
Abstract
Background: The Gender-Equity Model for liver Allocation corrected by serum sodium (GEMA-Na) and the Model for End-stage Liver Disease 3.0 (MELD 3.0) could amend sex disparities for accessing liver transplantation (LT). We aimed to assess these inequities in Spain and to compare the performance of GEMA-Na and MELD 3.0.
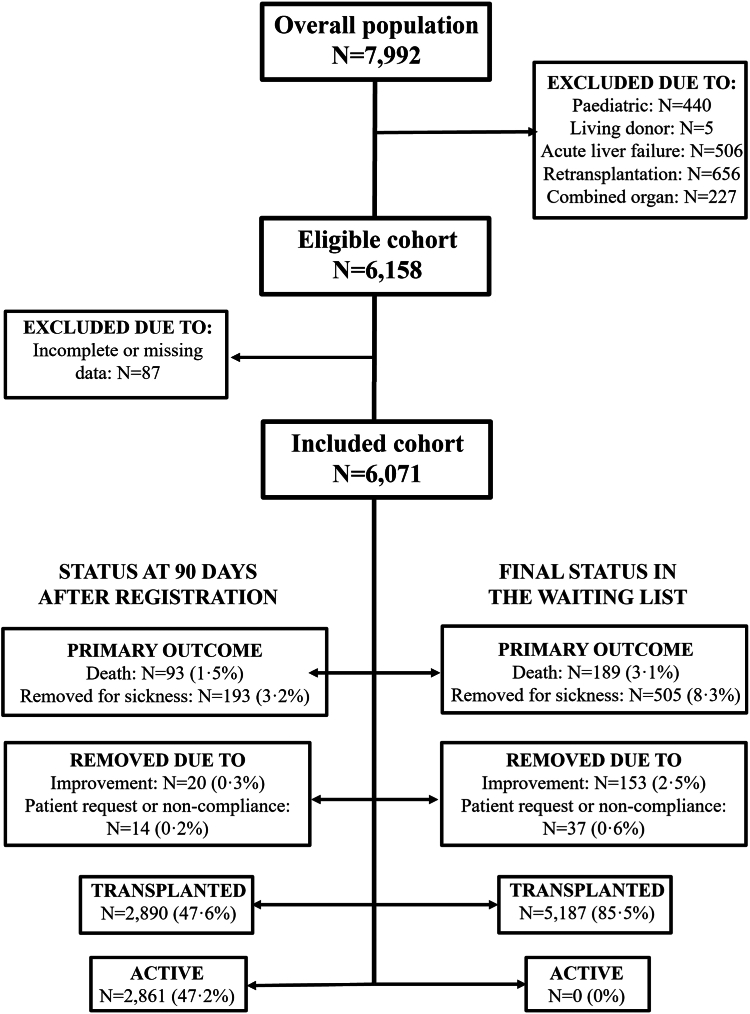
Methods: Nationwide cohort study including adult patients listed for a first elective LT (January 2016-December 2021). The primary outcome was mortality or delisting for sickness within the first 90 days. Independent predictors of the primary outcome were evaluated using multivariate Cox's regression with adjusted relative risks (RR) and 95% confidence intervals (95% CI). The discrimination of GEMA-Na and MELD 3.0was assessed using Harrell c-statistics (Hc).
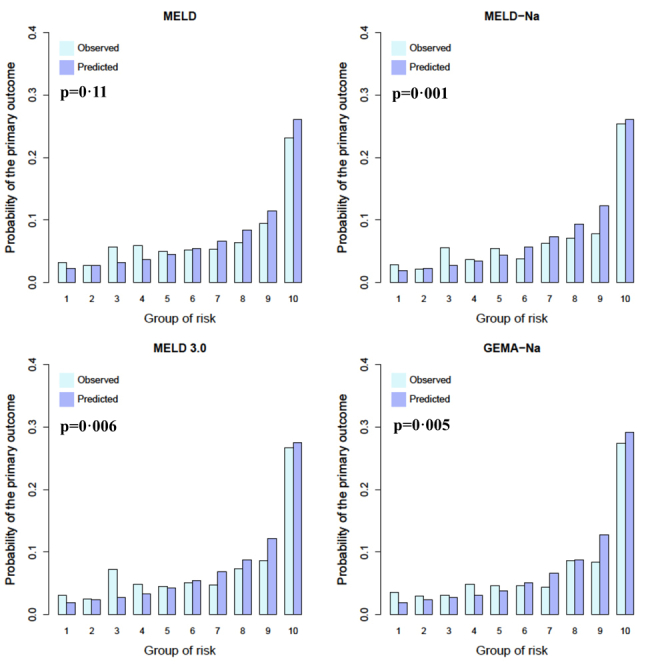
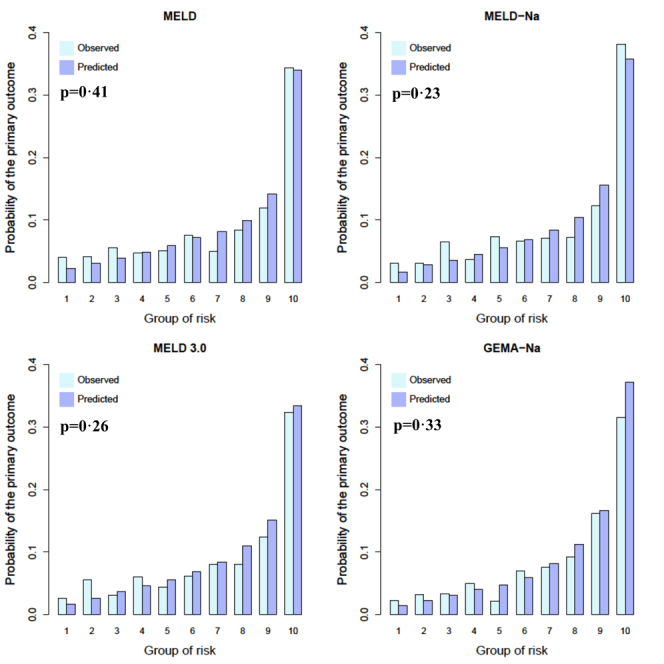
Findings: The study included 6071 patients (4697 men and 1374 women). Mortality or delisting for clinical deterioration occurred in 286 patients at 90 days (4.7%). Women had reduced access to LT (83.7% vs. 85.9%; p = 0.037) and increased risk of mortality or delisting for sickness at 90 days (adjusted RR = 1.57 [95% CI 1.09-2.28]; p = 0.017). Female sex remained as an independent risk factor when using MELD or MELD-Na but lost its significance in the presence of GEMA-Na or MELD 3.0. Among patients included for reasons other than tumours (n = 3606; 59.4%), GEMA-Na had Hc = 0.753 (95% CI 0.715-0.792), which was higher than MELD 3.0 (Hc = 0.726 [95% CI 0.686-0.767; p = 0.001), showing both models adequate calibration.
Interpretation: GEMA-Na and MELD 3.0 might correct sex disparities for accessing LT, but GEMA-Na provides more accurate predictions of waiting list outcomes and could be considered the standard of care for waiting list prioritization.
Funding: Instituto de Salud Carlos III, Agencia Estatal de Investigación (Spain), and European Union.
Keywords: Allocation; Equity; Liver transplantation; Sex; Urgency.
© 2024 The Author(s).
Conflict of interest statement
MLR-P has received lecture fees from Chiesi and Advanz Pharma, outside the present work. RM-M has received lecture fees from Chiesi, outside the present work. JC has received lecture fees from Chiesi and Astellas, outside the present work. All other authors declare no competing interests.
Figures
References
-
- Verna E.C., Lai J.C. Time for action to address the persistent sex-based disparity in liver transplant access. JAMA Surg. 2020;155(7):545–547. - PubMed
LinkOut - more resources
Full Text Sources
