

Neuropsychiatric involvement in systemic lupus erythematosus contributes to organ damage beyond the nervous system: a post-hoc analysis of 5 phase III randomized clinical trials
- PMID: 39115551
- PMCID: PMC11343782
- DOI: 10.1007/s00296-024-05667-5
Neuropsychiatric involvement in systemic lupus erythematosus contributes to organ damage beyond the nervous system: a post-hoc analysis of 5 phase III randomized clinical trials
Abstract
Objective: To investigate the association between neuropsychiatric systemic lupus erythematosus (NPSLE) and SLICC/ACR damage index (SDI) items, especially non-neuropsychiatric items.
Methods: Baseline data from five phase III trials (BLISS-52, BLISS-76, BLISS-SC, BLISS-NEA, EMBRACE) were analysed. NPSLE involvement was defined as NP BILAG A/B/C/D (n = 272); NP BILAG E denoted non-neuropsychiatric SLE (n = 3273). We employed multivariable logistic regression analysis adjusting for age, sex, disease duration, and ethnicity.
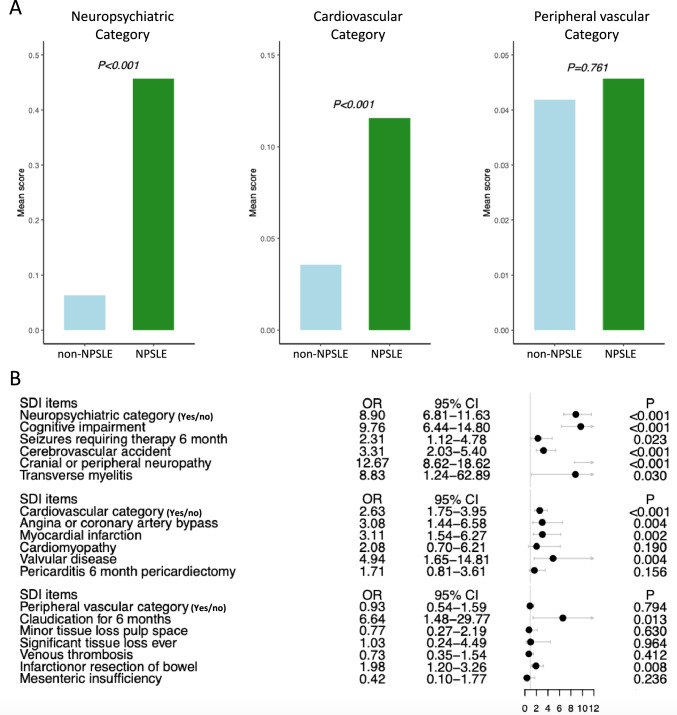
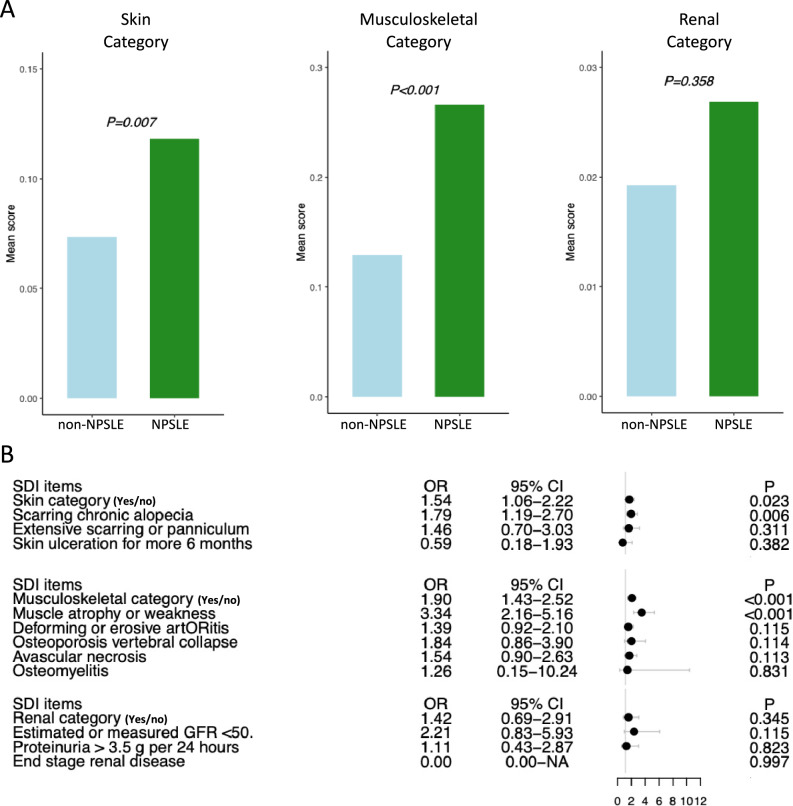
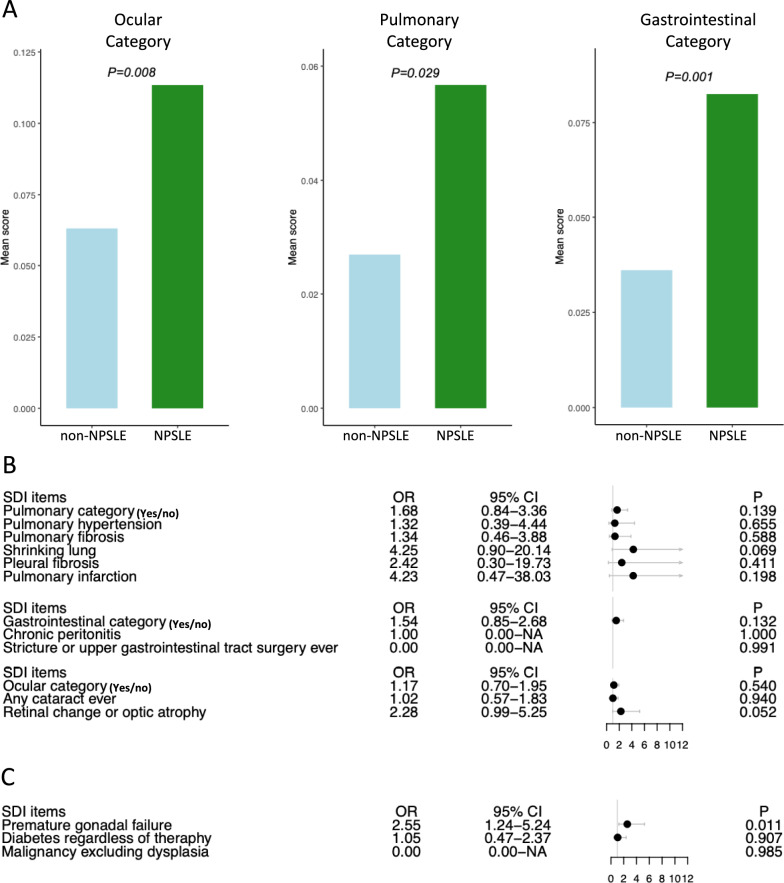
Results: The median (IQR) and mean ± SD SDI scores were 0 (0-1) and 0.62 ± 1.09. Compared with the non-neuropsychiatric SLE group, NPSLE patients were more likely to develop damage (adjusted (a)OR = 2.86; 95% CI = 2.28-3.59). This held true also after suppression of the NP SDI items (aOR = 1.70; 95% CI = 1.36-2.12). Beyond the neuropsychiatric domain, NPSLE was associated with damage in the cardiovascular (aOR = 2.63; 95% CI = 1.75-3.95), musculoskeletal (aOR = 1.90; 95% CI = 1.43-2.52), and skin (aOR = 1.54; 95% CI = 1.06-2.22) SDI domains. Dissecting domains into items, NPSLE was associated with coronary artery disease (aOR = 3.08; 95% CI = 1.44-6.58), myocardial infraction (aOR = 3.11; 95% CI = 1.54-6.27), muscle atrophy (aOR = 3.34; 2.16-5.16), scarring alopecia (aOR = 1.79; 95% CI = 1.19-2.70), bowel infarction (aOR = 1.98; 95% CI = 1.20-3.26), retinopathy (aOR = 2.23; 95% CI = 1.15-4.32), and premature gonadal failure (aOR = 2.10; 95% CI = 1.11-3.90).
Conclusion: The intricate association between NPSLE and damage accrual extends beyond the nervous system to also comprise the musculoskeletal, skin, and cardiovascular organ systems.
Trial registration: ClinicalTrials.gov NCT00424476 NCT00410384 NCT01484496 NCT01345253 NCT01632241.
Keywords: Nervous system; Neuropsychiatric lupus; Outcomes; SLICC/ACR damage index; Systemic lupus erythematosus.
© 2024. The Author(s).
Conflict of interest statement
IP has received research funding and/or honoraria from Amgen, AstraZeneca, Aurinia, Bristol-Myers Squibb, Elli Lilly, Gilead, GlaxoSmithKline, Janssen, Novartis, Otsuka, and Roche. The other authors declare that they have no conflicts of interest related to this work. The funders had no role in the design of the study, the analyses or interpretation of data, or the writing of the manuscript.
Figures
References
-
- Nikolopoulos D, Kostopoulou M, Pieta A, Karageorgas T, Tseronis D, Chavatza K et al (2020) Evolving phenotype of systemic lupus erythematosus in Caucasians: low incidence of lupus nephritis, high burden of neuropsychiatric disease and increased rates of late-onset lupus in the ‘Attikon’cohort. Lupus 29(5):514–522. 10.1177/0961203320908932 10.1177/0961203320908932 - DOI - PMC - PubMed
-
- Nikolopoulos D, Cetrez N, Lindblom J, Palazzo L, Enman Y, Parodis I (2024) Patients with NPSLE experience poorer HRQoL and more fatigue than SLE patients with no neuropsychiatric involvement, irrespective of neuropsychiatric activity. Rheumatology. 10.1093/rheumatology/keae216 10.1093/rheumatology/keae216 - DOI - PMC - PubMed
-
- Hanly JG, Urowitz MB, Gordon C, Bae SC, Romero-Diaz J, Sanchez-Guerrero J et al (2020) Neuropsychiatric events in systemic lupus erythematosus: a longitudinal analysis of outcomes in an international inception cohort using a multistate model approach. Ann Rheum Dis 79(3):356–362. 10.1136/annrheumdis-2019-216150 10.1136/annrheumdis-2019-216150 - DOI - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
