

Planned Dental Extractions After Radiation Therapy
- PMID: 39115868
- PMCID: PMC11310846
- DOI: 10.1001/jamaoto.2024.2353
Planned Dental Extractions After Radiation Therapy
Abstract
Importance: Nonrestorable teeth are recommended to be extracted prior to radiation therapy (RT). Occasionally, preradiation extractions introduce unacceptable delays in treatment initiation. Planned dental extractions immediately postradiation presents an alternative strategy, though outcomes are uncertain.
Objective: To evaluate the feasibility and safety of dental extractions immediately postradiation.
Design, setting, and participants: A prospective cohort study including patients planned for curative-intent RT but unable or unwilling to proceed with 1 or more extractions recommended pretreatment was carried out. From January 2020 to September 2022, 58 patients were screened and 50 enrolled. The dental care was performed at a single academic department and the cancer care at regional centers. Analysis took place between September 22, 2023, and June 10, 2024.
Exposure: On completion of RT, patients were recommended to complete extractions as soon as feasible, and ideally within 4 months.
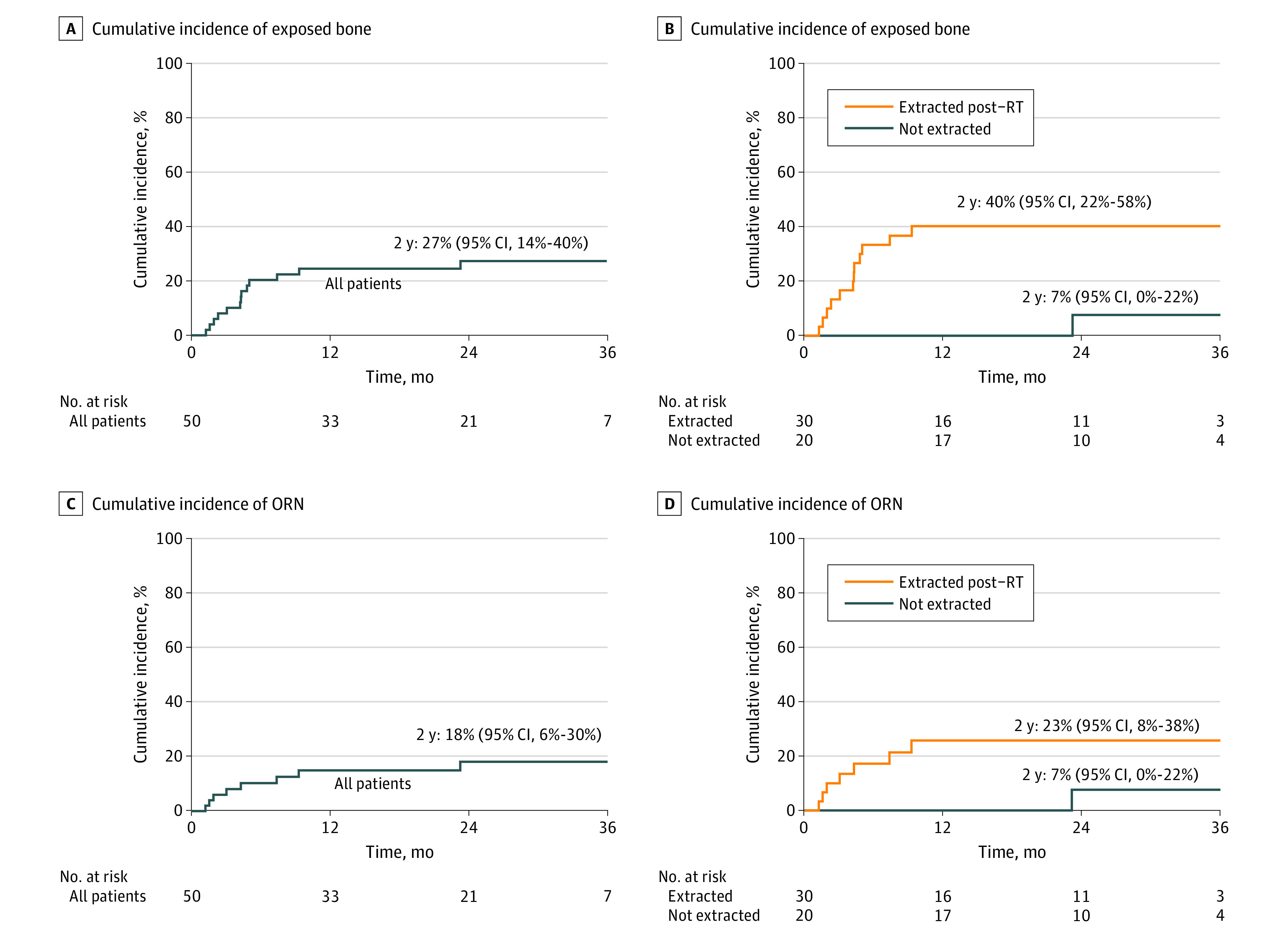
Main outcomes and measures: The primary end point was the actuarial cumulative incidence of exposed alveolar bone noted by any practitioner at any time after extraction, calculated using Gray method with death as a competing risk. As a pilot study, no formal power calculation was performed; resources allowed for 50 evaluable patients.
Results: Among the 50 participants enrolled, RT was nonoperative for 32 patients (64%) and postoperative for 18 patients (36%). Intensity-modulated RT (IMRT) was delivered in all patients. Of the 50 patients, 20 (40%) declined dental extractions immediately postradiation and the remaining 30 (60%) underwent a median (range) of 8.5 (1-28) extractions at a median (range) of 64.5 (13-152) days after RT. The median (IQR) follow-up for survivors without exposed bone was 26 (17-35) months from the end of RT. The 2-year cumulative incidence of any exposed bone was 27% (95% CI, 14%-40%). The 2-year incidence of exposed bone for those who underwent dental extractions immediately postradiation was 40% (95% CI, 22%-58%) and 7% (95% CI, 0%-22%) for those who did not. Of the 13 who developed exposed bone: 4 resolved, 1 was lost to follow-up, and 8 were confirmed as osteoradionecrosis.
Conclusions and relevance: This cohort study found that postradiation dental extractions incur considerable risk, even if performed within a 4-month window.
Conflict of interest statement
Figures

References
-
- Ratko TA, Douglas GW, de Souza JA, Belinson SE, Aronson N. Radiotherapy Treatments for Head and Neck Cancer Update. Agency for Healthcare Research and Quality; 2014. - PubMed
-
- Treister NS, Brennan MT, Sollecito TP, et al. Exposed bone in patients with head and neck cancer treated with radiation therapy: an analysis of the Observational Study of Dental Outcomes in Head and Neck Cancer Patients (OraRad). Cancer. 2022;128(3):487-496. doi: 10.1002/cncr.33948 - DOI - PMC - PubMed
-
- Brennan MT, Treister NS, Sollecito TP, et al. Tooth Failure Post-Radiotherapy in Head and Neck Cancer: Primary Report of the Clinical Registry of Dental Outcomes in Head and Neck Cancer Patients (OraRad) study. Int J Radiat Oncol Biol Phys. 2022;113(2):320-330. doi: 10.1016/j.ijrobp.2021.11.021 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
