

Leveraging machine learning to enhance postoperative risk assessment in coronary artery bypass grafting patients with unprotected left main disease: a retrospective cohort study
- PMID: 39116452
- PMCID: PMC11573096
- DOI: 10.1097/JS9.0000000000002032
Leveraging machine learning to enhance postoperative risk assessment in coronary artery bypass grafting patients with unprotected left main disease: a retrospective cohort study
Abstract
Background: Risk stratification for patients undergoing coronary artery bypass surgery (CABG) for left main coronary artery (LMCA) disease is essential for informed decision-making. This study explored the potential of machine learning (ML) methods to identify key risk factors associated with mortality in this patient group.
Methods: This retrospective cohort study was conducted on 866 patients from the Gulf Left Main Registry who presented between 2015 and 2019. The study outcome was hospital all-cause mortality. Various machine learning models [logistic regression, random forest (RF), k-nearest neighbor, support vector machine, naïve Bayes, multilayer perception, boosting] were used to predict mortality, and their performance was measured using accuracy, precision, recall, F1 score, and area under the receiver operator characteristic curve (AUC).
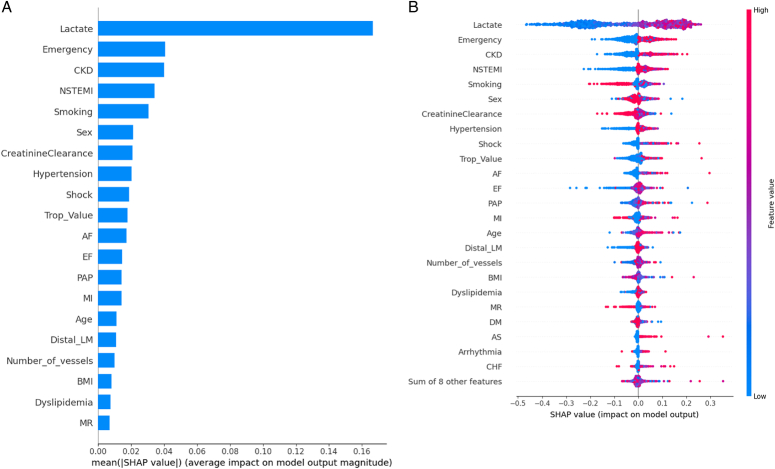
Results: Nonsurvivors had significantly greater EuroSCORE II values (1.84 (10.08-3.67) vs. 4.75 (2.54-9.53) %, P <0.001 for survivors and nonsurvivors, respectively). The EuroSCORE II score significantly predicted hospital mortality (OR: 1.13 (95% CI: 1.09-1.18), P <0.001), with an AUC of 0.736. RF achieved the best ML performance (accuracy=98, precision=100, recall=97, and F1 score=98). Explainable artificial intelligence using SHAP demonstrated the most important features as follows: preoperative lactate level, emergency surgery, chronic kidney disease (CKD), NSTEMI, nonsmoking status, and sex. QLattice identified lactate and CKD as the most important factors for predicting hospital mortality this patient group.
Conclusion: This study demonstrates the potential of ML, particularly the Random Forest, to accurately predict hospital mortality in patients undergoing CABG for LMCA disease and its superiority over traditional methods. The key risk factors identified, including preoperative lactate levels, emergency surgery, chronic kidney disease, NSTEMI, nonsmoking status, and sex, provide valuable insights for risk stratification and informed decision-making in this high-risk patient population. Additionally, incorporating newly identified risk factors into future risk-scoring systems can further improve mortality prediction accuracy.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
None.
Figures




References
-
- Pittams AP, Iddawela S, Zaidi S, et al. . Scoring systems for risk stratification in patients undergoing cardiac surgery. J Cardiothorac Vasc Anesth 2022;36:1148–1156. - PubMed
-
- Cai S, Li J, Gao J, et al. . Prediction models for postoperative delirium after cardiac surgery: Systematic review and critical appraisal. Int J Nurs Stud 2022;136:104340. - PubMed
-
- Stewart JJ, Turgeon R, Parker A, et al. . Comparison of risk-scoring systems for heparin-induced thrombocytopenia in cardiac surgery patients. Pharmacotherapy 2021;41:1033–1040. - PubMed
-
- Sabatine MS, Bergmark BA, Murphy SA, et al. . Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: an individual patient data meta-analysis. Lancet (London, England) 2021;398:2247–2257. - PubMed
-
- Gao F, Shan L, Wang C, et al. . Predictive ability of European Heart Surgery Risk Assessment System II (EuroSCORE II) and the Society of Thoracic Surgeons (STS) Score for in-hospital and medium-term mortality of patients undergoing coronary artery bypass grafting. Int J Gen Med 2021;14:8509–8519. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
