

Giant unruptured middle cerebral artery aneurysm revealed by intracranial hypertension: is a systematic decompressive hemicraniotomy mandatory?
- PMID: 39117892
- PMCID: PMC11310238
- DOI: 10.1007/s10143-024-02662-z
Giant unruptured middle cerebral artery aneurysm revealed by intracranial hypertension: is a systematic decompressive hemicraniotomy mandatory?
Abstract
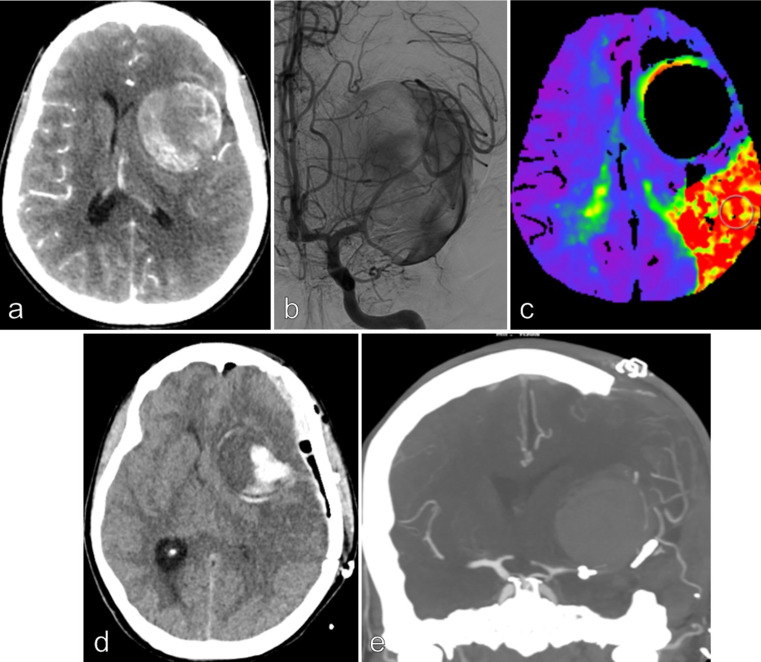
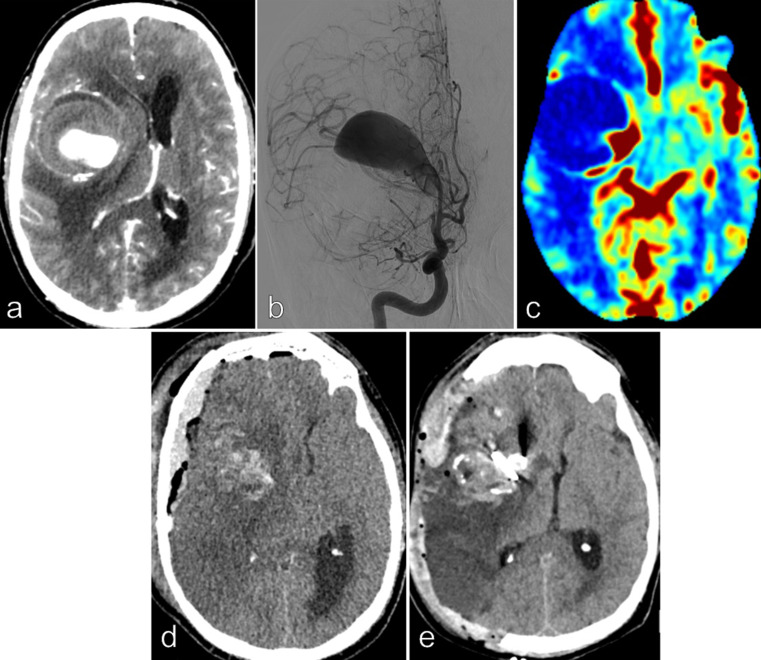
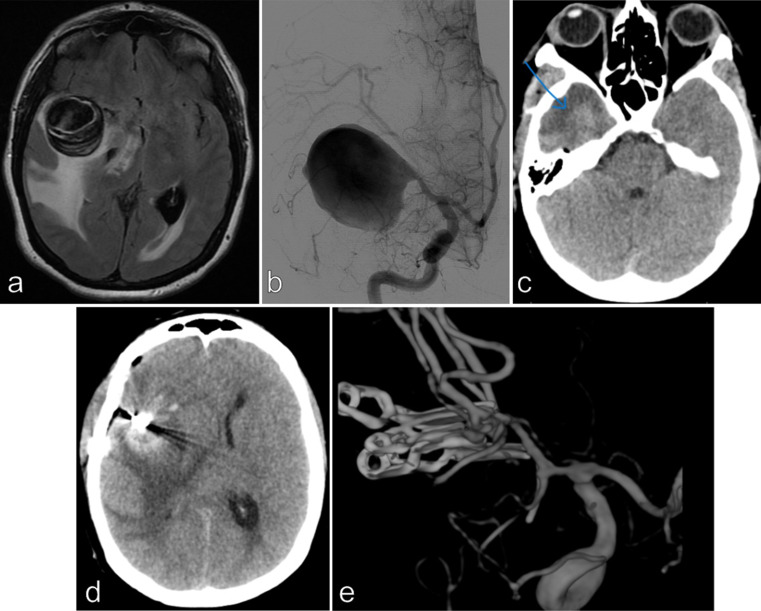
Our study aimed to evaluate the postoperative outcome of patients with unruptured giant middle cerebral artery (MCA) aneurysm revealed by intracranial hypertension associated to midline brain shift. From 2012 to 2022, among the 954 patients treated by a microsurgical procedure for an intracranial aneurysm, our study included 9 consecutive patients with giant MCA aneurysm associated to intracranial hypertension with a midline brain shift. Deep hypothermic circulatory flow reduction (DHCFR) with vascular reconstruction was performed in 4 patients and cerebral revascularization with aneurysm trapping was the therapeutic strategy in 5 patients. Early (< 7 days) and long term clinical and radiological monitoring was done. Good functional outcome was considered as mRS score ≤ 2 at 3 months. The mean age at treatment was 44 yo (ranged from 17 to 70 yo). The mean maximal diameter of the aneurysm was 49 mm (ranged from 33 to 70 mm). The mean midline brain shift was 8.6 mm (ranged from 5 to 13 mm). Distal MCA territory hypoperfusion was noted in 6 patients. Diffuse postoperative cerebral edema occurred in the 9 patients with a mean delay of 59 h and conducted to a postoperative neurological deterioration in 7 of them. Postoperative death was noted in 3 patients. Among the 6 survivors, early postoperative decompressive hemicraniotomy was required in 4 patients. Good functional outcome was noted in 4 patients. Complete aneurysm occlusion was noted in each patient at last follow-up. We suggest to discuss a systematic decompressive hemicraniotomy at the end of the surgical procedure and/or a partial temporal lobe resection at its beginning to reduce the consequences of the edema reaction and to improve the postoperative outcome of this specific subgroup of patients. A better intraoperative assessment of the blood flow might also reduce the occurrence of the reperfusion syndrome.
Keywords: Anastomosis; Bypass; Deep hypothermic circulatory flow arrest; Giant aneurysm; Mca; Microsurgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Aboukais R, Devalckeneer A, Boussemart P, Bourgeois P, Menovsky T, Leclerc X, Vinchon M, Lejeune JP (2022) Is malignant edema and hemorrhage after occlusion of high-flow arteriovenous malformation related to the size of feeding arteries and draining veins? Neurochirurgie 68:e1–e7. 10.1016/j.neuchi.2022.01.008 - DOI - PubMed
-
- Cagnazzo F, Mantilla D, Rouchaud A, Brinjikji W, Lefevre PH, Dargazanli C, Gascou G, Riquelme C, Perrini P, di Carlo D, Bonafe A, Costalat V (2018) Endovascular treatment of very large and giant intracranial aneurysms: comparison between reconstructive and deconstructive Techniques-A Meta-analysis. AJNR Am J Neuroradiol 39:852–858. 10.3174/ajnr.A5591 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
