

First Successful Treatment of a Patient with a Primary Immune Complex-Membranoproliferative Glomerulonephritis with Iptacopan: A Case Report
- PMID: 39118827
- PMCID: PMC11309753
- DOI: 10.1159/000540013
First Successful Treatment of a Patient with a Primary Immune Complex-Membranoproliferative Glomerulonephritis with Iptacopan: A Case Report
Abstract
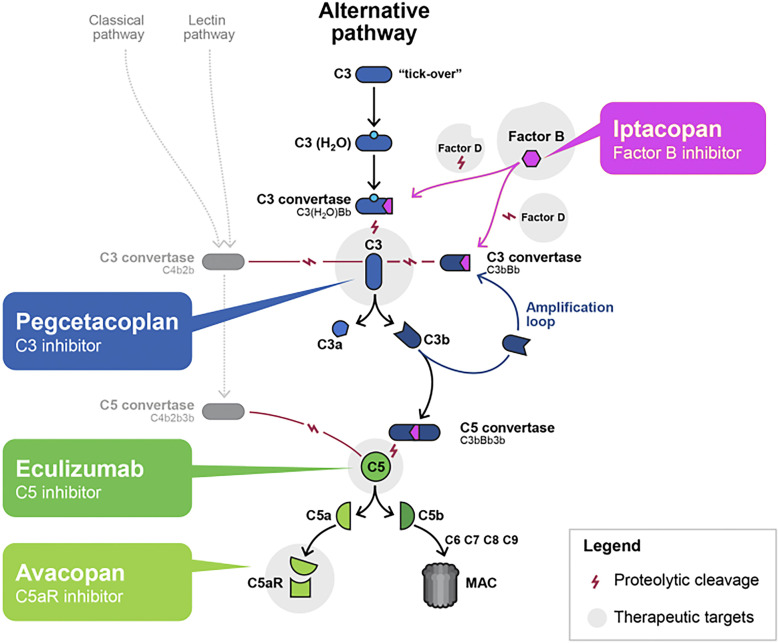
Introduction: Nowadays, there is insufficient evidence for the recommendation of management patients with a primary membranoproliferative glomerulonephritis (MPGN). A better understanding of the pathogenesis has led to the reclassification of primary MPGN and distinction into the two main entities of either primary immune complex-MPGN or C3 glomerulopathy. Both entities share overlapping pathophysiological features with complement alternative pathway (AP) dysregulation. Iptacopan is an oral inhibitor of the complement factor B that effectively blocks the complement AP.
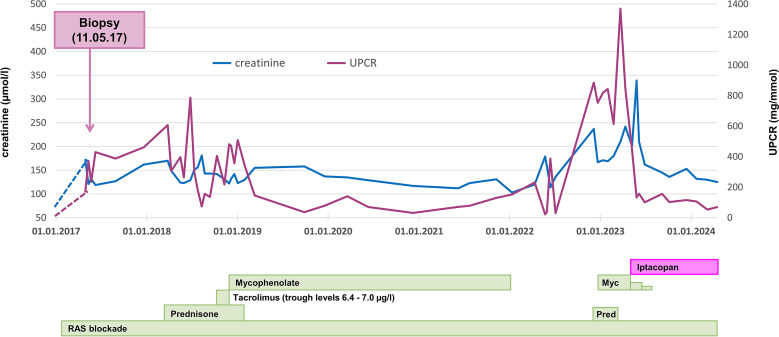
Case presentation: We report the first successful treatment of a 47-year-old man suffering from a primary immune complex-MPGN with iptacopan. So far established immunosuppressive therapies with prednisone and mycophenolate mofetil failed to control the current flare of the disease, mainly presenting with impaired kidney function and proteinuria within the nephrotic range. However, 3 months after starting the treatment with iptacopan urine protein-creatinine ratio decreased impressively to a level of 100-150 mg/mmol. Thereafter, low-level proteinuria and kidney function remained stable during follow-up. Do date, the treatment with iptacopan is continued as a monotherapy and is well tolerated.
Conclusion: To the best of our knowledge, this is the first case report which suggests that iptacopan may be an interesting treatment option for primary immune complex-MPGN.
Keywords: Alternative complement pathway; Complement factor B inhibitor; Iptacopan; Membranoproliferative glomerulonephritis; Primary immune complex-associated.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors of this manuscript declare no conflicts of interest as described by Karger Case Reports in Nephrology and Dialysis. This study received funding from Novartis Pharma AG, Basel, Switzerland as indicated within the funding section.
Figures
References
-
- Fakhouri F, Fremeaux-Bacchi V, Noel LH, Cook HT, Pickering MC. C3 glomerulopathy: a new classification. Nat Rev Nephrol. 2010;6(8):494–9. - PubMed
-
- Noris M, Donadelli R, Remuzzi G. Autoimmune abnormalities of the alternative complement pathway in membranoproliferative glomerulonephritis and C3 glomerulopathy. Pediatr Nephrol. 2019;34(8):1311–23. - PubMed
-
- Rovin BH, Adler SG, Barratt J, Bridoux F, Burdge KA, Chan TM, et al. . Executive summary of the KDIGO 2021 guideline for the management of glomerular diseases. Kidney Int. 2021;100(4):753–79. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
