

ICU-Electroencephalogram Unit Improves Outcome in Status Epilepticus Patients: A Retrospective Before-After Study
- PMID: 39120451
- PMCID: PMC11469622
- DOI: 10.1097/CCM.0000000000006393
ICU-Electroencephalogram Unit Improves Outcome in Status Epilepticus Patients: A Retrospective Before-After Study
Abstract
Objectives: Continuous electroencephalogram (cEEG) monitoring is recommended for status epilepticus (SE) management in ICU but is still underused due to resource limitations and inconclusive evidence regarding its impact on outcome. Furthermore, the term "continuous monitoring" often implies continuous recording with variable intermittent review. The establishment of a dedicated ICU-electroencephalogram unit may fill this gap, allowing cEEG with nearly real-time review and multidisciplinary management collaboration. This study aimed to evaluate the effect of ICU-electroencephalogram unit establishing on SE outcome and management.
Design: Single-center retrospective before-after study.
Setting: Neuro-ICU of a Swiss academic tertiary medical care center.
Patients: Adult patients treated for nonhypoxic SE between November 1, 2015, and December 31, 2023.
Interventions: None.
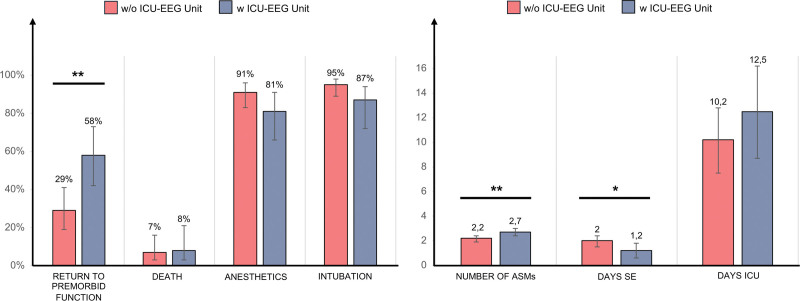
Measurement and main results: Data from all SE patients were assessed, comparing those treated before and after ICU-electroencephalogram unit introduction. Primary outcomes were return to premorbid neurologic function, ICU mortality, SE duration, and ICU SE management. Secondary outcomes were SE type and etiology. Two hundred seven SE patients were included, 149 (72%) before and 58 (38%) after ICU-electroencephalogram unit establishment. ICU-electroencephalogram unit introduction was associated with increased detection of nonconvulsive SE ( p = 0.003) and SE due to acute symptomatic etiology ( p = 0.019). Regression analysis considering age, comorbidities, SE etiology, and SE semeiology revealed a higher chance of returning to premorbid neurologic function ( p = 0.002), reduced SE duration ( p = 0.024), and a shift in SE management with increased use of antiseizure medications ( p = 0.007) after ICU-electroencephalogram unit introduction.
Conclusions: Integrating neurology expertise in the ICU setting through the establishment of an ICU-electroencephalogram unit with nearly real-time cEEG review, shortened SE duration, and increased likelihood of returning to premorbid neurologic function, with an increased number of antiseizure medications used. Further studies are warranted to validate these findings and assess long-term prognosis.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Misirocchi is supported by the 2023 International Federation of Clinical Neurophysiology Research Fellowship Grant. Dr. Kleinschmidt has received honoraria for consulting from Abbvie, Eli Lilly, Lundbeck, Mitsubishi Tanabe, Novartis, and TEVA that were paid to a teaching and research fund at the University Hospital Geneva. Dr. Seeck is a shareholder of Epilog NV (Ghent, Belgium); she received grants from the Swiss National Science Foundation (163398, CRS115-180365). Dr. De Stefano was supported by the Swiss National Science Foundation (163398, CRS115-180365) and is supported by the 2022 Swiss League Against Epilepsy Research Support Prize; she is supported by the Swiss National Science Foundation (163398, CRS115-180365) and is supported by the 2022 Swiss League Against Epilepsy Research Support Prize. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Rosenthal ES: Seizures, status epilepticus, and continuous eeg in the intensive care unit. Continuum (Minneap Minn) 2021; 27:1321–1343 - PubMed
-
- Brophy GM, Bell R, Claassen J, et al. ; Neurocritical Care Society Status Epilepticus Guideline Writing Committee: Guidelines for the evaluation and management of status epilepticus. Neurocrit Care 2012; 17:3–23 - PubMed
-
- Claassen J, Taccone FS, Horn P, et al. ; Neurointensive Care Section of the European Society of Intensive Care Medicine: Recommendations on the use of EEG monitoring in critically ill patients: Consensus statement from the neurointensive care section of the ESICM. Intensive Care Med 2013; 39:1337–1351 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
