

Efficacy and safety of insomnia treatment with lemborexant in older adults: analyses from three clinical trials
- PMID: 39120786
- PMCID: PMC11408585
- DOI: 10.1007/s40266-024-01135-8
Efficacy and safety of insomnia treatment with lemborexant in older adults: analyses from three clinical trials
Abstract
Background: Insomnia is more common as people age. Several common hypnotics used to treat insomnia often do not adequately alleviate sleep issues in older adults and may be associated with negative residual effects such as an increased risk of falls, cognitive impairment, automobile accidents, and lack of response to auditory stimuli. The objective of these analyses of three clinical studies was to investigate the efficacy and safety of the dual orexin-receptor antagonist lemborexant (LEM) in older adults.
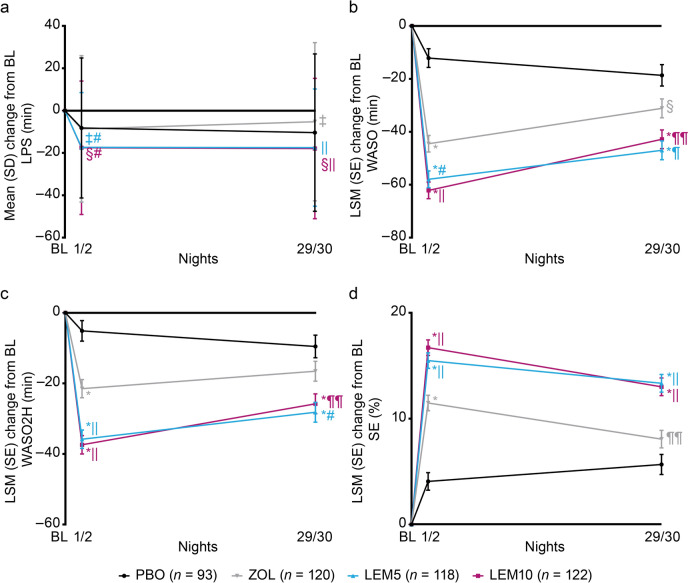
Methods: Study E2006-G000-304 (Study 304; NCT02783729) was a randomized, double-blind, placebo (PBO)-controlled, active-comparator trial where subjects with insomnia disorder received LEM 5 mg (LEM5), LEM 10 mg (LEM10), zolpidem tartrate extended-release 6.25 mg (ZOL), or PBO for 30 days. In crossover Study E2006-E044-106 (Study 106; NCT02583451), healthy subjects (good sleepers) received LEM 2.5 mg, LEM5, LEM10, or PBO for eight nights or zopiclone on days 1 and 8 (and PBO on days 2-7). In crossover Study E2006-A001-108 (Study 108; NCT03008447), healthy subjects received a single dose of LEM5, LEM10, PBO, or ZOL. Sleep assessments included polysomnography-based latency to persistent sleep (LPS), wake after sleep onset (WASO), WASO in the second half of the night (WASO2H), sleep efficiency, postural stability, middle-of-the-night and next-day cognitive performance, middle-of-the-night auditory awakening threshold and return-to-sleep latency, and driving performance.
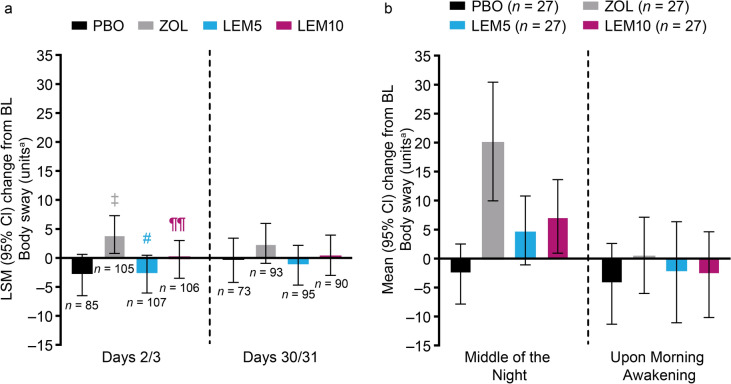
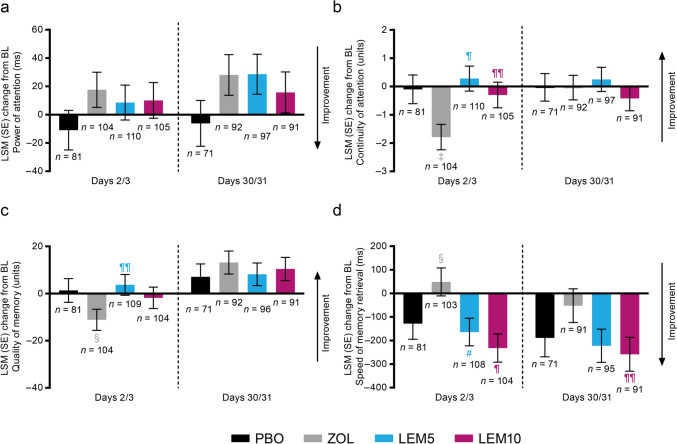
Results: Overall, 453 of 1006 (45%; Study 304), 24 of 48 (50%; Study 106), and 28 of 56 (50%; Study 108) subjects were aged ≥ 65 years. In Study 304, LEM decreased (improved) LPS, WASO, and WASO2H from baseline more than ZOL and PBO; subjects treated with LEM had greater increases in sleep efficiency (improved) than with ZOL or PBO. In both Studies 304 and 108, postural stability was not impaired at waketime in subjects who received LEM compared with PBO. At waketime, LEM did not impair memory compared with PBO. In Study 108, following middle-of-the-night awakening, LEM and ZOL did not affect subjects' ability to awaken to auditory stimuli; LEM did not affect tests of memory and attention. In Study 106, LEM did not impair next-day driving performance in healthy elderly compared with PBO. LEM was well tolerated in subjects aged ≥ 65 years.
Conclusions: LEM provided benefits on sleep variables without next-morning residual effects in subjects aged ≥ 65 years, supporting LEM as a treatment option for older adults with insomnia.
Trial registration numbers and dates of registration: Study 304: ClinicalTrials.gov identifier, NCT02783729, date of registration, 26 May 2016. Study 106: ClinicalTrials.gov identifier, NCT02583451, date of registration, 22 October 2015. Study 108: ClinicalTrials.gov identifier, NCT03008447, date of registration, 2 January 2017.
Plain language summary
The prevalence of insomnia increases with age; however, some hypnotics used for treating insomnia do not adequately resolve sleep problems in older adults and may be associated with adverse residual effects. Specifically, some hypnotics pose safety concerns in this population of patients who are generally more vulnerable to treatment-related effects, including increasing the risk of falls, risks of cognitive impairment, automobile accidents, and unresponsiveness to auditory stimuli. Safer and more effective insomnia medications are needed to reduce sleep problems with improved side-effect profiles. This analysis of lemborexant clinical studies conducted in adult subjects at least 65 years old found the drug to be effective without impairing memory, attention or balance the following day compared with placebo. These subjects were normal sleepers (for age) or had insomnia disorder. Furthermore, lemborexant was not associated with impaired ability to drive the next morning or awaken to loud middle-of-the-night sounds. Lemborexant was well tolerated in these older adults, similar to findings for adults aged at least 18 years. These findings indicate that lemborexant may be an appropriate treatment option for insomnia in older adults.
© 2024. The Author(s).
Conflict of interest statement
Dr. Gotfried has received research support and/or speaker fees from Eisai Inc., Idorsia, Jazz Pharmaceuticals, and Merck. Dr. Auerbach declares he has no conflicts of interest. Dr. Dang-Vu has been a consultant and/or speaker for and/or has received research support from Eisai Inc., Jazz Pharmaceuticals, and Paladin Labs. Dr. Mishima has been a consultant and/or speaker for and/or has received research support from Eisai Co., Ltd., MSD, Nobelpharma, and Takeda Pharmaceutical Limited. Drs Kumar and Moline are employees of Eisai Inc. Dr. Malhotra is a former employee of Eisai Inc.
Figures

References
-
- Foley DJ, Monjan AA, Brown SL, Simonsick EM, Wallace RB, Blazer DG. Sleep complaints among elderly persons: an epidemiologic study of three communities. Sleep. 1995;18(6):425–32. 10.1093/sleep/18.6.425. - PubMed
-
- Crowley K. Sleep and sleep disorders in older adults. Neuropsychol Rev. 2011;21(1):41–53. 10.1007/s11065-010-9154-6. - PubMed
-
- Schroeck JL, Ford J, Conway EL, Kurtzhalts KE, Gee ME, Vollmer KA, et al. Review of safety and efficacy of sleep medicines in older adults. Clin Ther. 2016;38(11):2340–72. 10.1016/j.clinthera.2016.09.010. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
