

Inactivated rabies-based Lassa fever virus vaccine candidate LASSARAB protects nonhuman primates from lethal disease
- PMID: 39122759
- PMCID: PMC11315998
- DOI: 10.1038/s41541-024-00930-z
Inactivated rabies-based Lassa fever virus vaccine candidate LASSARAB protects nonhuman primates from lethal disease
Abstract
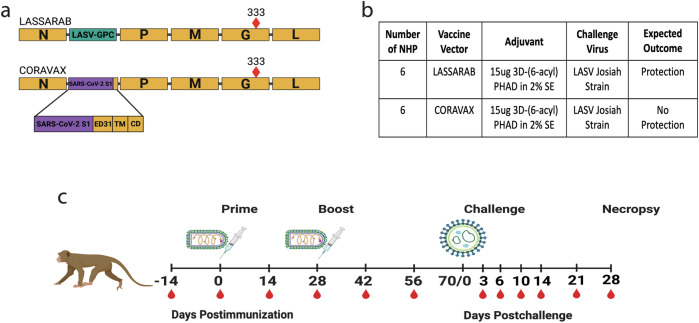
Lassa fever virus (LASV), a member of the Arenavirus family, is the etiological agent of Lassa fever, a severe hemorrhagic disease that causes considerable morbidity and mortality in the endemic areas of West Africa. LASV is a rodent-borne CDC Tier One biological threat agent and is on the World Health Organization's (WHO) Priority Pathogen list. Currently, no FDA-licensed vaccines or specific therapeutics are available. Here, we describe the efficacy of a deactivated rabies virus (RABV)-based vaccine encoding the glycoprotein precursor (GPC) of LASV (LASSARAB). Nonhuman primates (NHPs) were administered a two-dose regimen of LASSARAB or an irrelevant RABV-based vaccine to serve as a negative control. NHPs immunized with LASSARAB developed strong humoral responses to LASV-GPC. Upon challenge, NHPs vaccinated with LASSARAB survived to the study endpoint, whereas NHPs in the control group did not. This study demonstrates that LASSARAB is a worthy candidate for continued development.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures







References
-
- Ogbu, O., Ajuluchukwu, E. & Uneke, C. J. Lassa fever in West African sub-region: an overview. J. Vector Borne Dis.44, 1–11 (2007). - PubMed
Grants and funding
- HHSN272201700082C/AI/NIAID NIH HHS/United States
- T32 AI134646/AI/NIAID NIH HHS/United States
- R01AI105204/Division of Intramural Research, National Institute of Allergy and Infectious Diseases (Division of Intramural Research of the NIAID)
- 2T32AI134646/Division of Intramural Research, National Institute of Allergy and Infectious Diseases (Division of Intramural Research of the NIAID)
LinkOut - more resources
Full Text Sources
