

Deep learning versus manual morphology-based embryo selection in IVF: a randomized, double-blind noninferiority trial
- PMID: 39122964
- PMCID: PMC11564097
- DOI: 10.1038/s41591-024-03166-5
Deep learning versus manual morphology-based embryo selection in IVF: a randomized, double-blind noninferiority trial
Abstract
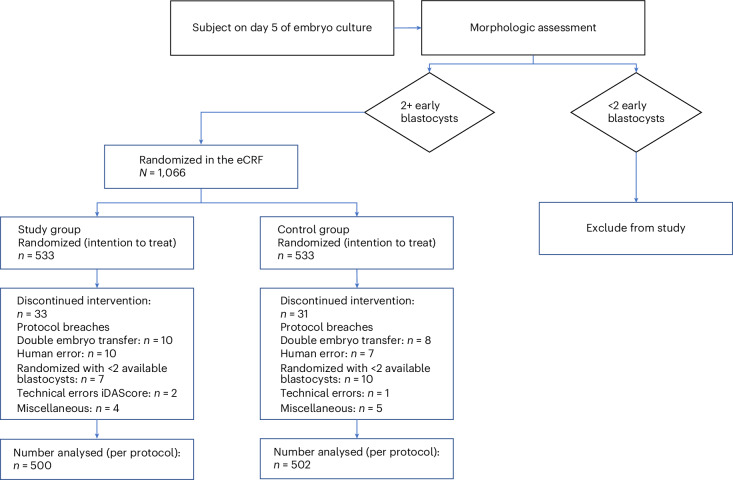
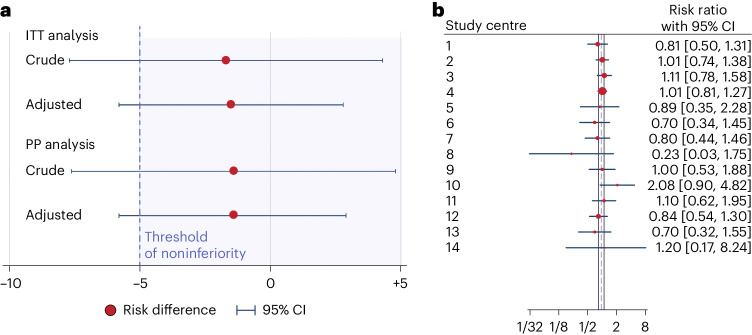
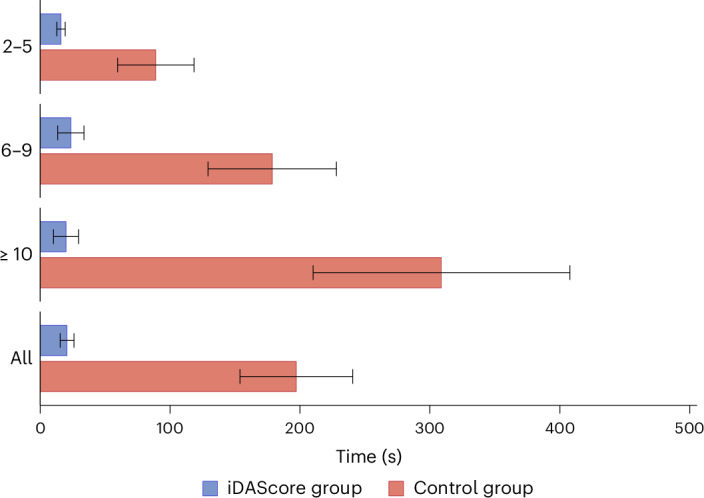
To assess the value of deep learning in selecting the optimal embryo for in vitro fertilization, a multicenter, randomized, double-blind, noninferiority parallel-group trial was conducted across 14 in vitro fertilization clinics in Australia and Europe. Women under 42 years of age with at least two early-stage blastocysts on day 5 were randomized to either the control arm, using standard morphological assessment, or the study arm, employing a deep learning algorithm, intelligent Data Analysis Score (iDAScore), for embryo selection. The primary endpoint was a clinical pregnancy rate with a noninferiority margin of 5%. The trial included 1,066 patients (533 in the iDAScore group and 533 in the morphology group). The iDAScore group exhibited a clinical pregnancy rate of 46.5% (248 of 533 patients), compared to 48.2% (257 of 533 patients) in the morphology arm (risk difference -1.7%; 95% confidence interval -7.7, 4.3; P = 0.62). This study was not able to demonstrate noninferiority of deep learning for clinical pregnancy rate when compared to standard morphology and a predefined prioritization scheme. Australian New Zealand Clinical Trials Registry (ANZCTR) registration: 379161 .
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- Lang, K. et al. Artificial intelligence-supported screen reading versus standard double reading in the mammography screening with Artificial Intelligence trial (MASAI): a clinical safety analysis of a randomized, controlled, non-inferiority, single-blinded, screening accuracy study. Lancet Oncol.24, 936–944 (2023). - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
