

Pulse Pressure as a Hemodynamic Parameter in Preeclampsia with Severe Features Accompanied by Fetal Growth Restriction
- PMID: 39124585
- PMCID: PMC11312723
- DOI: 10.3390/jcm13154318
Pulse Pressure as a Hemodynamic Parameter in Preeclampsia with Severe Features Accompanied by Fetal Growth Restriction
Abstract
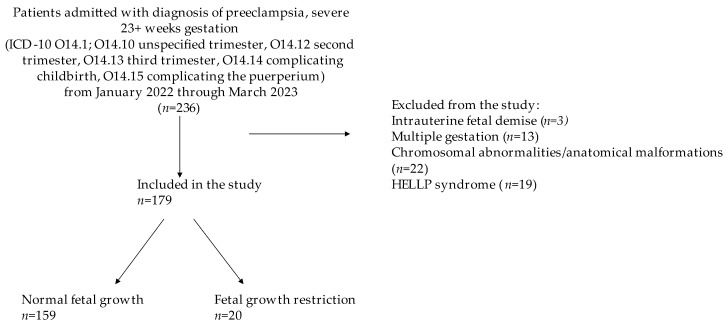
Background: Modern management of preeclampsia can be optimized by tailoring the targeted treatment of hypertension to an individual's hemodynamic profile. Growing evidence suggests different phenotypes of preeclampsia, including those with a hyperdynamic profile and those complicated by uteroplacental insufficiency. Fetal growth restriction (FGR) is believed to be a result of uteroplacental insufficiency. There is a paucity of research examining the characteristics of patients with severe preeclampsia who do and who do not develop FGR. We aimed to elucidate which hemodynamic parameters differed between these two groups. Methods: All patients admitted to a single referral center with severe preeclampsia were identified. Patients were included if they had a live birth at 23 weeks of gestation or higher. Multiple gestations and pregnancies complicated by fetal congenital anomalies and/or HELLP syndrome were excluded. FGR was defined as a sonographic estimation of fetal weight (EFW) < 10th percentile or abdominal circumference (AC) < 10th percentile. Results: There were 76% significantly lower odds of overall pulse pressure upon admission for those with severe preeclampsia comorbid with FGR (aOR = 0.24, 95% CI = 0.07-0.83). Advanced gestational age on admission was associated with lower odds of severely abnormal labs and severely elevated diastolic blood pressure in preeclampsia also complicated by FGR. Conclusions: Subtypes of preeclampsia with and without FGR may be hemodynamically evaluated by assessing pulse pressure on admission.
Keywords: fetal growth restriction; fetal health; gynecology; hemodynamics; maternal health; obstetrics; preeclampsia with severe features; pulse pressure.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Fetal growth restriction and intra-uterine growth restriction: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians.Eur J Obstet Gynecol Reprod Biol. 2015 Oct;193:10-8. doi: 10.1016/j.ejogrb.2015.06.021. Epub 2015 Jul 2. Eur J Obstet Gynecol Reprod Biol. 2015. PMID: 26207980
-
Severity of fetal growth restriction stratified according to maternal obesity.J Matern Fetal Neonatal Med. 2022 May;35(10):1886-1890. doi: 10.1080/14767058.2020.1773427. Epub 2020 Jun 1. J Matern Fetal Neonatal Med. 2022. PMID: 32482116
-
Impact of chemotherapy during pregnancy on fetal growth.J Matern Fetal Neonatal Med. 2022 Dec;35(26):10314-10323. doi: 10.1080/14767058.2022.2128645. Epub 2022 Oct 6. J Matern Fetal Neonatal Med. 2022. PMID: 36202393
-
Fetal Growth Restriction: A Comprehensive Review of Major Guidelines.Obstet Gynecol Surv. 2023 Nov;78(11):690-708. doi: 10.1097/OGX.0000000000001203. Obstet Gynecol Surv. 2023. PMID: 38134339 Review.
-
Fetal Growth Restriction: Does an Integrated Maternal Hemodynamic-Placental Model Fit Better?Reprod Sci. 2021 Sep;28(9):2422-2435. doi: 10.1007/s43032-020-00393-2. Epub 2020 Nov 19. Reprod Sci. 2021. PMID: 33211274 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
