

Prenatal Diagnosis, Course and Outcome of Patients with Truncus Arteriosus Communis
- PMID: 39124733
- PMCID: PMC11313530
- DOI: 10.3390/jcm13154465
Prenatal Diagnosis, Course and Outcome of Patients with Truncus Arteriosus Communis
Abstract
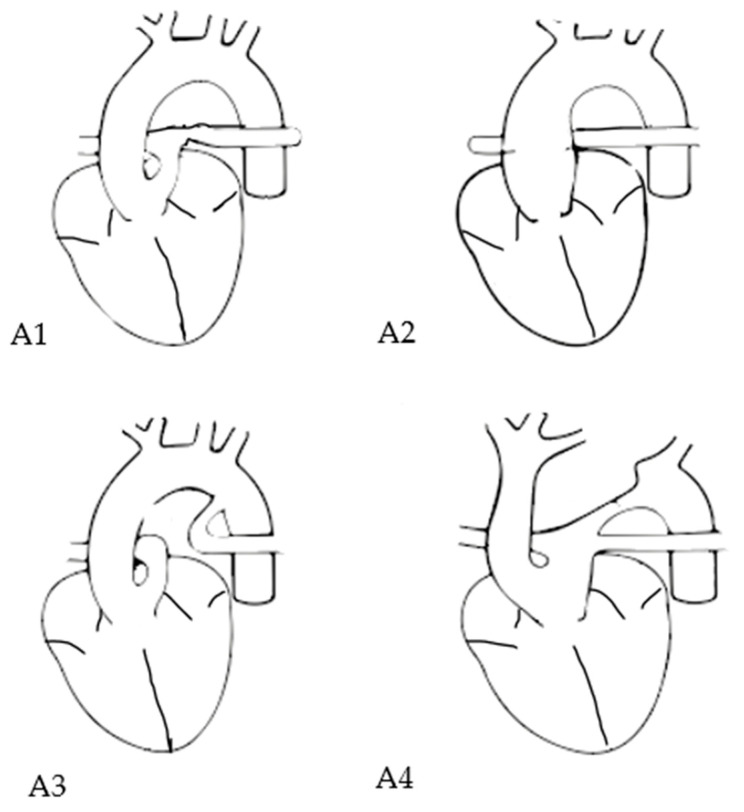
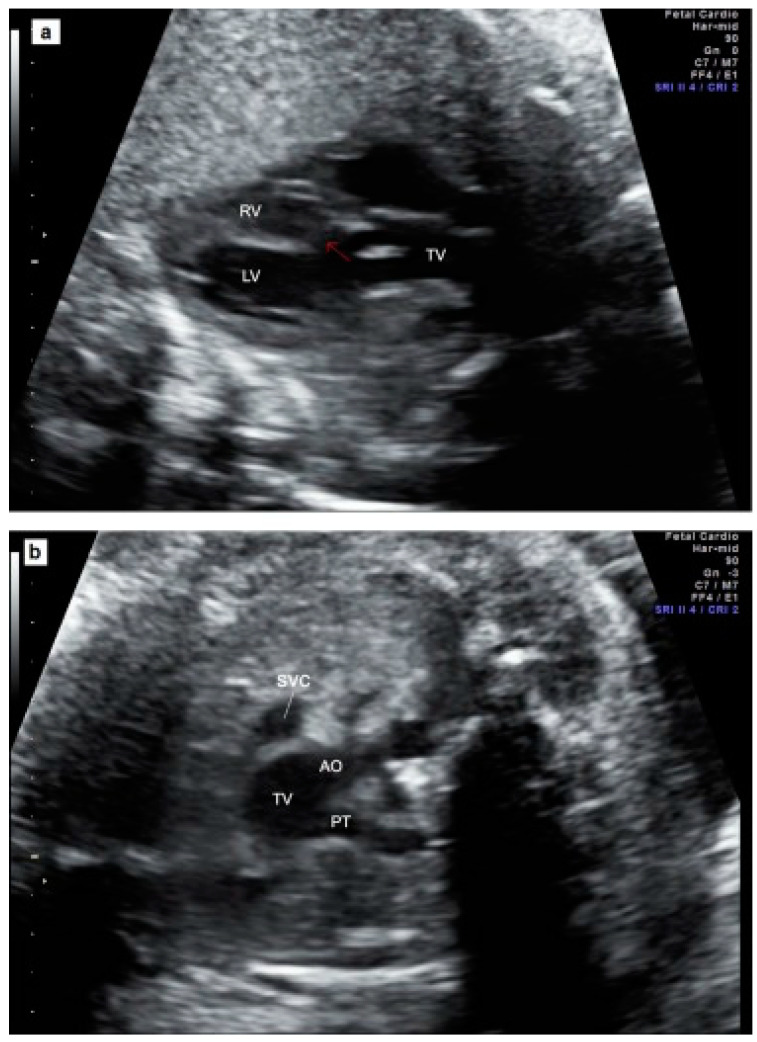
Background: The objective of our study was to assess the prenatal course, associated anomalies and postnatal outcome and the predictive value of various prenatal parameters for survival in prenatally diagnosed cases of truncus arteriosus communis (TAC). Methods: We evaluated cases from four centers between 2008 and 2021. Results: In 37/47 cases (78.7%), classification into a Van Praagh sbtype was possible, most had TAC type A1 (18/37 = 48.6%). In 33/47 (70.2%) with available valve details on common trunk valve, most presented with tricuspid valves (13/33 = 39.4%). In the overall sample, 14/47 (29.8%) had relevant insufficiency, and 8/47 (17%) had stenosis. In total, 37/47 (78.7%) underwent karyotyping, with 15/37 (40.5%) showing abnormal results, mainly 22q11.2 microdeletion (9/37 = 24.3%). Overall, 17/47 (36.2%) had additional extracardiac anomalies (17/47 = 36.2%). Additional intracardiac anomalies were present in 30/47 (63.8%), or 32/47 (68.1%) if coronary anomalies were included. Four (8.5%) had major defects. Two (4.3%) intrauterine deaths occurred, in 10 (21.3%) cases, the parents opted for termination, predominantly in non-isolated cases (8/10 = 80.0%). A total of 35/47 (74.5%) were born alive at 39 (35-41) weeks. Three (8.6%) pre-surgical deaths occurred in non-isolated cases. In 32/35 (91.4%), correction surgery was performed. The postoperative survival rate was 84.4% (27/32) over a median follow-up of 51.5 months. Initial intervention was performed 16 (1-71) days postpartum, and 22/32 (68.8%) required re-intervention. Regarding prenatal outcome-predicting parameters, no significant differences were identified between the survivor and non-survivor groups. Conclusions: There exist limited outcome data for TAC. To our knowledge, this is the largest multicenter, prenatal cohort with an intention-to-treat survival rate of almost 85%.
Keywords: congenital heart disease; prenatal diagnosis; prenatal outcome prediction; truncus arteriosus communis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
LinkOut - more resources
Full Text Sources
