

Low-Voltage Area Ablation in Addition to Pulmonary Vein Isolation in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis
- PMID: 39124807
- PMCID: PMC11313645
- DOI: 10.3390/jcm13154541
Low-Voltage Area Ablation in Addition to Pulmonary Vein Isolation in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis
Abstract
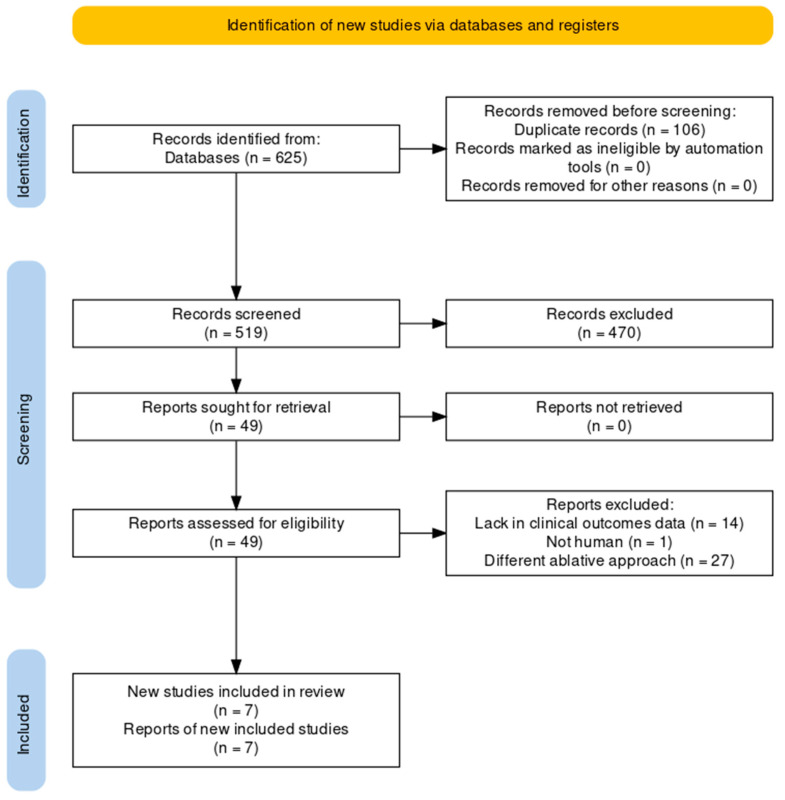
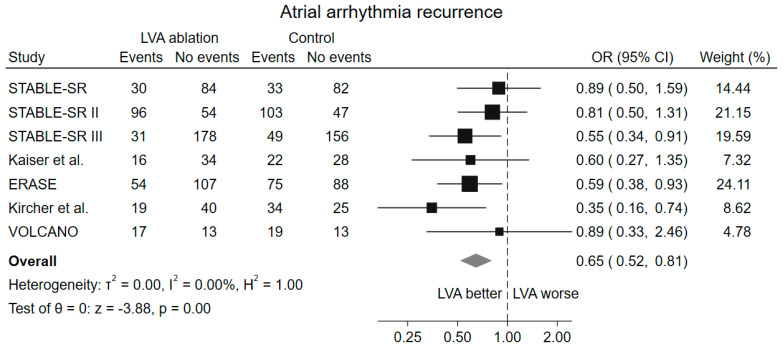
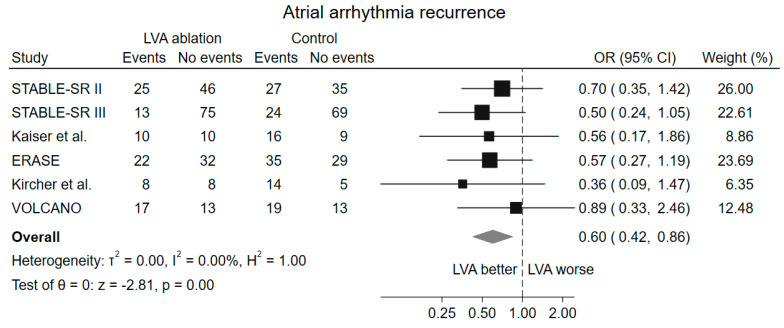
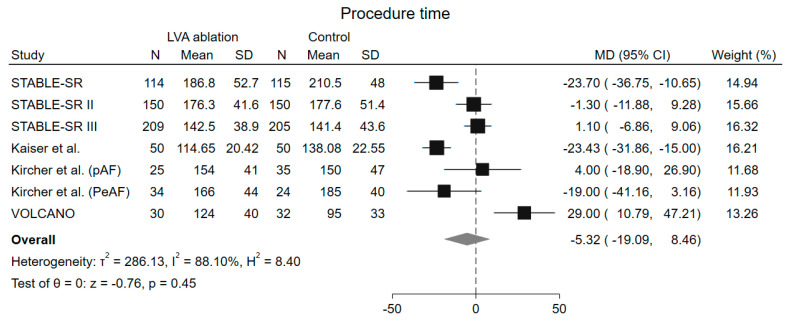
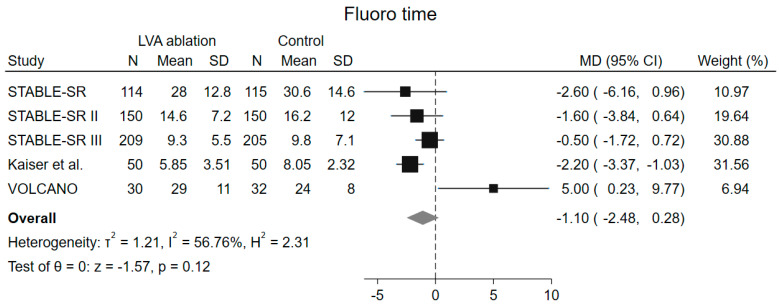
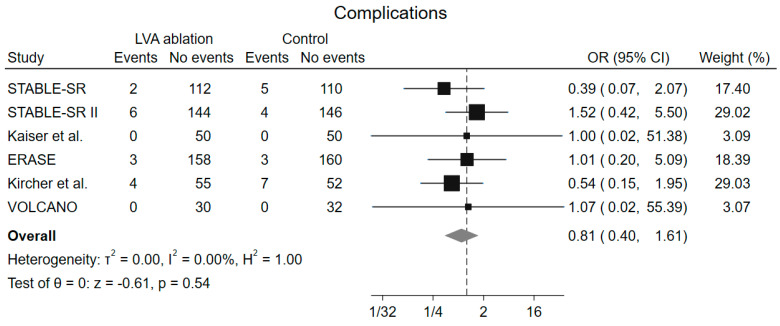
Background: Low-voltage area (LVA) ablation, in addition to pulmonary vein isolation (PVI), has been proposed as a new strategy in patients with atrial fibrillation (AF), but clinical trials have shown conflicting results. We performed a systematic review and meta-analysis to assess the impact of LVA ablation in patient undergoing AF ablation (PROSPERO-registered CRD42024537696). Methods: Randomized clinical trials investigating the role of LVA ablation in addition to PVI in patients with AF were searched on PubMed, Embase, and the Cochrane Library from inception to 22 April 2024. Primary outcome was atrial arrhythmia recurrence after the first AF ablation procedure. Secondary endpoints included procedure time, fluoroscopy time, and procedure-related complication rate. Sensitivity analysis including only patients with LVA demonstration at mapping and multiple subgroups analyses were also performed. Results: 1547 patients from 7 studies were included. LVA ablation in addition to PVI reduced atrial arrhythmia recurrence (odds ratio [OR] 0.65, 95% confidence interval [CI] 0.52-0.81, p < 0.001) with a number needed to treat to prevent recurrence of 10. No difference in procedure time (mean difference [MD] -5.32 min, 95% CI -19.01-8.46 min, p = 0.45), fluoroscopy time (MD -1.10 min, 95% CI -2.48-0.28 min, p = 0.12) and complication rate (OR 0.81, 95% CI 0.40-1.61, p = 0.54) was observed. Consistent results were demonstrated when considering only patients with LVA during mapping and in prespecified subgroups for AF type (paroxysmal vs. persistent), multicentric vs. monocentric trial, and ablation strategy in control group. Conclusions: In patients with AF, ablation of LVAs in addition to PVI reduces atrial arrhythmia recurrence without a significant increase in procedure time, fluoroscopy time, or complication rate.
Keywords: atrial fibrillation; catheter ablation; low-voltage area; metanalysis; paroxysmal atrial fibrillation; persistent atrial fibrillation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Arbelo E., Aktaa S., Bollmann A., D’Avila A., Drossart I., Dwight J., Hills M.T., Hindricks G., Kusumoto F.M., Lane D.A., et al. Quality Indicators for the Care and Outcomes of Adults with Atrial Fibrillation: Task Force for the Development of Quality Indicators in Atrial Fibrillation of the European Heart Rhythm Association (EHRA) of the European Society of Cardiology (ESC): Developed in Collaboration with the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), and the Latin-American Heart Rhythm Society (LAHRS) EP Eur. 2021;23:494–495. doi: 10.1093/EUROPACE/EUAA253. - DOI - PubMed
-
- Nabauer M., Oeff M., Gerth A., Wegscheider K., Buchholz A., Haeusler K.G., Hanrath P., Meinertz T., Ravens U., Sprenger C., et al. Prognostic Markers of All-Cause Mortality in Patients with Atrial Fibrillation: Data from the Prospective Long-Term Registry of the German Atrial Fibrillation NETwork (AFNET) EP Eur. 2021;23:1903–1912. doi: 10.1093/europace/euab113. - DOI - PubMed
-
- Haïssaguerre M., Jaïs P., Shah D.C., Takahashi A., Hocini M., Quiniou G., Garrigue S., Le Mouroux A., Le Métayer P., Clémenty J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N. Engl. J. Med. 1998;339:659–666. doi: 10.1056/NEJM199809033391003. - DOI - PubMed
-
- Joglar J.A., Chung M.K., Armbruster A.L., Benjamin E.J., Chyou J.Y., Cronin E.M., Deswal A., Eckhardt L.L., Goldberger Z.D., Gopinathannair R., et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149:e1–e156. doi: 10.1161/CIR.0000000000001193. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
