

NAFLD (MASLD)/NASH (MASH): Does It Bother to Label at All? A Comprehensive Narrative Review
- PMID: 39126031
- PMCID: PMC11313354
- DOI: 10.3390/ijms25158462
NAFLD (MASLD)/NASH (MASH): Does It Bother to Label at All? A Comprehensive Narrative Review
Abstract
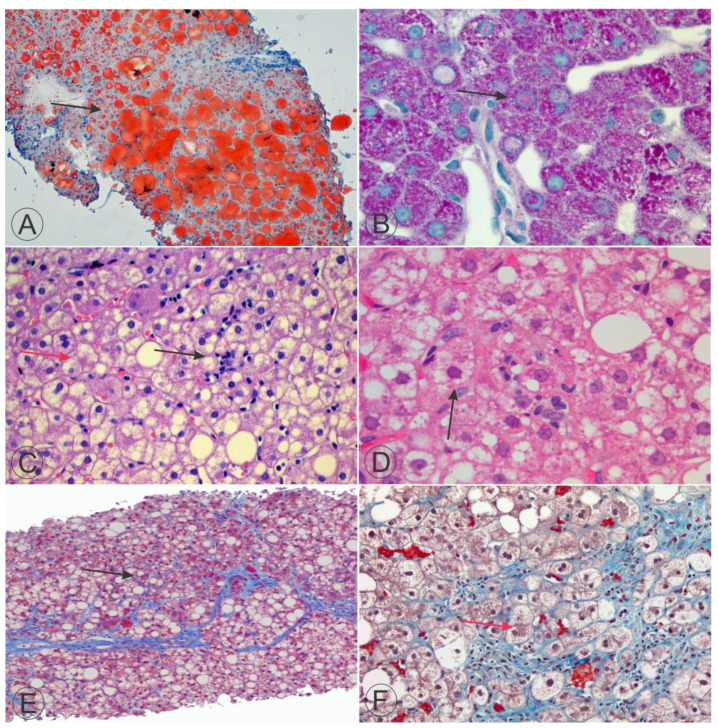
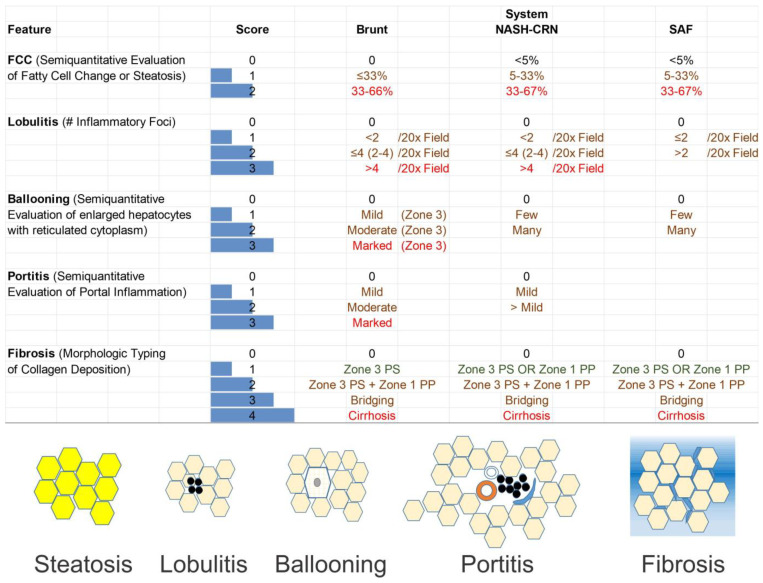
Nonalcoholic fatty liver disease (NAFLD), or metabolic dysfunction-associated steatotic liver disease (MASLD), is a liver condition that is linked to overweight, obesity, diabetes mellitus, and metabolic syndrome. Nonalcoholic steatohepatitis (NASH), or metabolic dysfunction-associated steatohepatitis (MASH), is a form of NAFLD/MASLD that progresses over time. While steatosis is a prominent histological characteristic and recognizable grossly and microscopically, liver biopsies of individuals with NASH/MASH may exhibit several other abnormalities, such as mononuclear inflammation in the portal and lobular regions, hepatocellular damage characterized by ballooning and programmed cell death (apoptosis), misfolded hepatocytic protein inclusions (Mallory-Denk bodies, MDBs), megamitochondria as hyaline inclusions, and fibrosis. Ballooning hepatocellular damage remains the defining feature of NASH/MASH. The fibrosis pattern is characterized by the initial expression of perisinusoidal fibrosis ("chicken wire") and fibrosis surrounding the central veins. Children may have an alternative form of progressive NAFLD/MASLD characterized by steatosis, inflammation, and fibrosis, mainly in Rappaport zone 1 of the liver acinus. To identify, synthesize, and analyze the scientific knowledge produced regarding the implications of using a score for evaluating NAFLD/MASLD in a comprehensive narrative review. The search for articles was conducted between 1 January 2000 and 31 December 2023, on the PubMed/MEDLINE, Scopus, Web of Science, and Cochrane databases. This search was complemented by a gray search, including internet browsers (e.g., Google) and textbooks. The following research question guided the study: "What are the basic data on using a score for evaluating NAFLD/MASLD?" All stages of the selection process were carried out by the single author. Of the 1783 articles found, 75 were included in the sample for analysis, which was implemented with an additional 25 articles from references and gray literature. The studies analyzed indicated the beneficial effects of scoring liver biopsies. Although similarity between alcoholic steatohepatitis (ASH) and NASH/MASH occurs, some patterns of hepatocellular damage seen in alcoholic disease of the liver do not happen in NASH/MASH, including cholestatic featuring steatohepatitis, alcoholic foamy degeneration, and sclerosing predominant hyaline necrosis. Generally, neutrophilic-rich cellular infiltrates, prominent hyaline inclusions and MDBs, cholestasis, and obvious pericellular sinusoidal fibrosis should favor the diagnosis of alcohol-induced hepatocellular injury over NASH/MASH. Multiple grading and staging methods are available for implementation in investigations and clinical trials, each possessing merits and drawbacks. The systems primarily used are the Brunt, the NASH CRN (NASH Clinical Research Network), and the SAF (steatosis, activity, and fibrosis) systems. Clinical investigations have utilized several approaches to link laboratory and demographic observations with histology findings with optimal platforms for clinical trials of rapidly commercialized drugs. It is promising that machine learning procedures (artificial intelligence) may be critical for developing new platforms to evaluate the benefits of current and future drug formulations.
Keywords: MASH; MASLD; NAFLD; NASH; classification; liver; nomenclature; scores; taxonomy.
Conflict of interest statement
The author declares no conflict of interest.
Figures
Similar articles
-
Histopathology, grading and staging of nonalcoholic fatty liver disease.Minerva Gastroenterol Dietol. 2018 Mar;64(1):28-38. doi: 10.23736/S1121-421X.17.02445-X. Epub 2017 Sep 25. Minerva Gastroenterol Dietol. 2018. PMID: 28948754 Review.
-
EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD): Executive Summary.Diabetologia. 2024 Nov;67(11):2375-2392. doi: 10.1007/s00125-024-06196-3. Diabetologia. 2024. PMID: 38869512 Free PMC article.
-
Liver biopsy-based validation, confirmation and comparison of the diagnostic performance of established and novel non-invasive steatotic liver disease indexes: Results from a large multi-center study.Metabolism. 2023 Oct;147:155666. doi: 10.1016/j.metabol.2023.155666. Epub 2023 Jul 30. Metabolism. 2023. PMID: 37527759
-
EASL-EASD-EASO Clinical Practice Guidelines on the Management of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD).Obes Facts. 2024;17(4):374-444. doi: 10.1159/000539371. Epub 2024 Jun 7. Obes Facts. 2024. PMID: 38852583 Free PMC article.
-
Impact of Weight Loss on Metabolic Dysfunction Associated Steatohepatitis and Hepatic Fibrosis.Curr Diab Rep. 2025 Feb 18;25(1):23. doi: 10.1007/s11892-025-01579-1. Curr Diab Rep. 2025. PMID: 39964660 Review.
Cited by
-
Metabolic Dysfunction-Associated Steatotic Liver Disease Induced by Microplastics: An Endpoint in the Liver-Eye Axis.Int J Mol Sci. 2025 Mar 21;26(7):2837. doi: 10.3390/ijms26072837. Int J Mol Sci. 2025. PMID: 40243419 Free PMC article. Review.
-
Potential mechanisms and therapeutic prospects of the association between Helicobacter pylori infection and metabolic dysfunction-associated steatohepatitis.World J Hepatol. 2025 Jan 27;17(1):101798. doi: 10.4254/wjh.v17.i1.101798. World J Hepatol. 2025. PMID: 39871896 Free PMC article.
-
Distinct Biomarker Profiles of B-Cell Activation in Metabolic and Viral Hepatic Fibrosis.Int J Mol Sci. 2025 Jun 20;26(13):5942. doi: 10.3390/ijms26135942. Int J Mol Sci. 2025. PMID: 40649718 Free PMC article.
-
Clopidogrel ameliorates high-fat diet-induced hepatic steatosis in mice through activation of the AMPK signaling pathway and beyond.Front Pharmacol. 2024 Oct 23;15:1496639. doi: 10.3389/fphar.2024.1496639. eCollection 2024. Front Pharmacol. 2024. PMID: 39508046 Free PMC article.
-
Targeting Metabolism: Innovative Therapies for MASLD Unveiled.Int J Mol Sci. 2025 Apr 25;26(9):4077. doi: 10.3390/ijms26094077. Int J Mol Sci. 2025. PMID: 40362316 Free PMC article. Review.
References
-
- Sergi C., Chiu B., Feulefack J., Shen F., Chiu B. Usefulness of resveratrol supplementation in decreasing cardiometabolic risk factors comparing subjects with metabolic syndrome and healthy subjects with or without obesity: Meta-analysis using multinational, randomised, controlled trials. Arch. Med. Sci. Atheroscler. Dis. 2020;5:e98–e111. doi: 10.5114/amsad.2020.95884. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
