

Acute Hyperglycemia-Induced Injury in Myocardial Infarction
- PMID: 39126075
- PMCID: PMC11313474
- DOI: 10.3390/ijms25158504
Acute Hyperglycemia-Induced Injury in Myocardial Infarction
Abstract
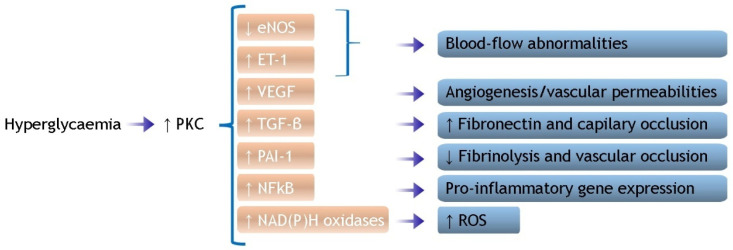
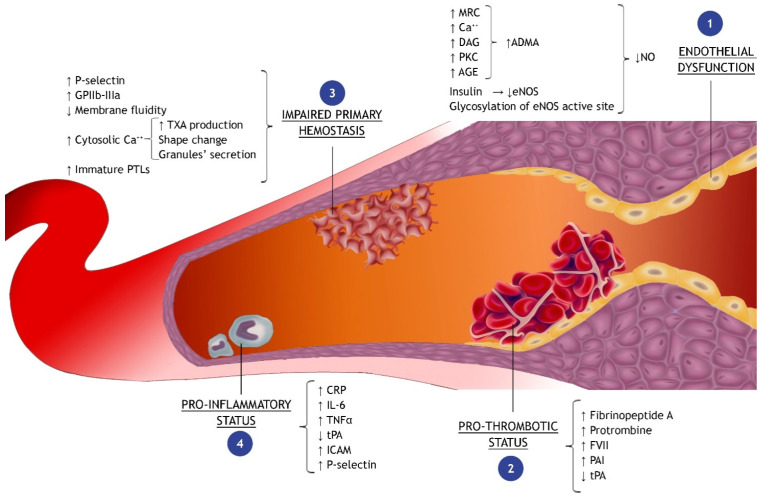
Acute hyperglycemia is a transient increase in plasma glucose level (PGL) frequently observed in patients with ST-elevation myocardial infarction (STEMI). The aim of this review is to clarify the molecular mechanisms whereby acute hyperglycemia impacts coronary flow and myocardial perfusion in patients with acute myocardial infarction (AMI) and to discuss the consequent clinical and prognostic implications. We conducted a comprehensive literature review on the molecular causes of myocardial damage driven by acute hyperglycemia in the context of AMI. The negative impact of high PGL on admission recognizes a multifactorial etiology involving endothelial function, oxidative stress, production of leukocyte adhesion molecules, platelet aggregation, and activation of the coagulation cascade. The current evidence suggests that all these pathophysiological mechanisms compromise myocardial perfusion as a whole and not only in the culprit coronary artery. Acute hyperglycemia on admission, regardless of whether or not in the context of a diabetes mellitus history, could be, thus, identified as a predictor of worse myocardial reperfusion and poorer prognosis in patients with AMI. In order to reduce hyperglycemia-related complications, it seems rational to pursue in these patients an adequate and quick control of PGL, despite the best pharmacological treatment for acute hyperglycemia still remaining a matter of debate.
Keywords: coagulation; coronary flow; diabetes mellitus; endothelium; inflammation.
Conflict of interest statement
Giuseppe Biondi-Zoccai has consulted for Aleph, Amarin, Balmed, Cardionovum, Crannmedical, Endocore Lab, Eukon, Guidotti, Innovheart, Meditrial, Menarini, Microport, Opsens Medical, Terumo, and Translumina, outside the present work. The authors declare no conflict of interest.
Figures

References
-
- Deedwania P., Kosiborod M., Barrett E., Ceriello A., Isley W., Mazzone T., Raskin P. Hyperglycemia and acute coronary syndrome: A scientific statement from the american heart association diabetes committee of the council on nutrition, physical activity, and metabolism. Circulation. 2008;117:1610–1619. doi: 10.1161/CIRCULATIONAHA.107.188629. - DOI - PubMed
-
- Kosuge M., Kimura K., Kojima S., Sakamoto T., Matsui K., Ishihara M., Asada Y., Tei C., Miyazaki S., Sonoda M., et al. Effects of glucose abnormalities on in-hospital outcome after coronary intervention for acute myocardial infarction. Circ. J. 2005;69:375–379. doi: 10.1253/circj.69.375. - DOI - PubMed
-
- Kosiborod M., Rathore S.S., Inzucchi S.E., Masoudi F.A., Wang Y., Havranek E.P., Krumholz H.M. Admission glucose and mortality in elderly patients hospitalized with acute myocardial infarction: Implications for patients with and without recognized diabetes. Circulation. 2005;111:3078–3086. doi: 10.1161/CIRCULATIONAHA.104.517839. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
