

Unraveling the impact of therapeutic drug monitoring via machine learning for patients with sepsis
- PMID: 39127039
- PMCID: PMC11384951
- DOI: 10.1016/j.xcrm.2024.101681
Unraveling the impact of therapeutic drug monitoring via machine learning for patients with sepsis
Abstract
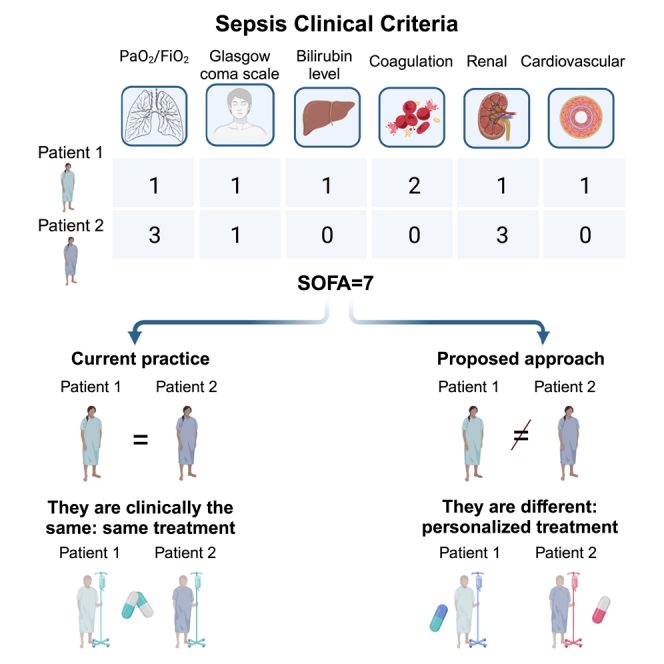
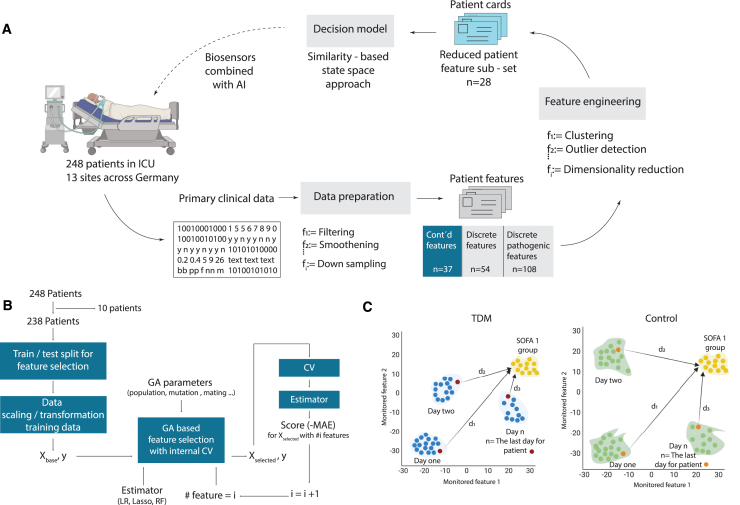
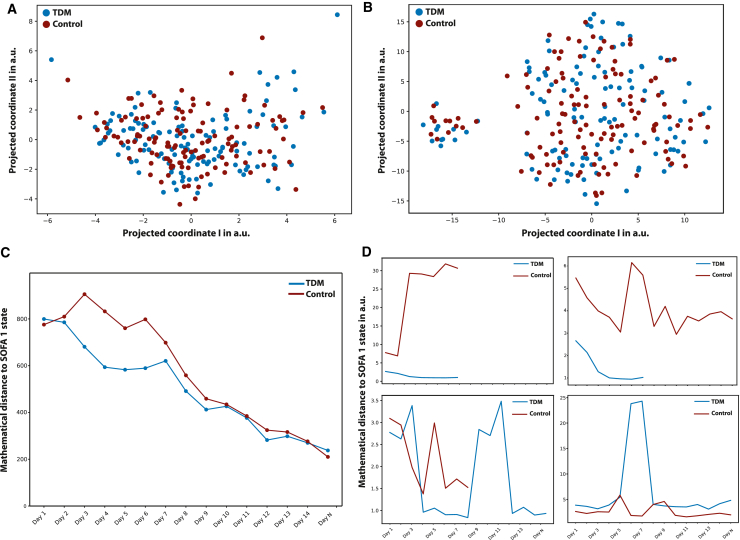
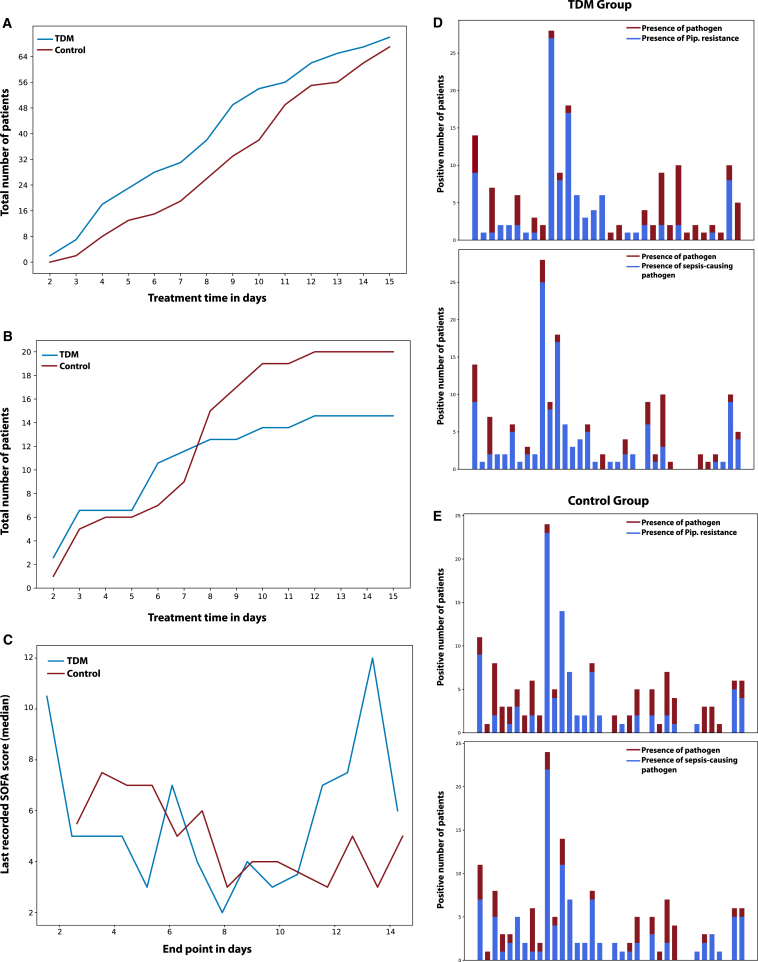
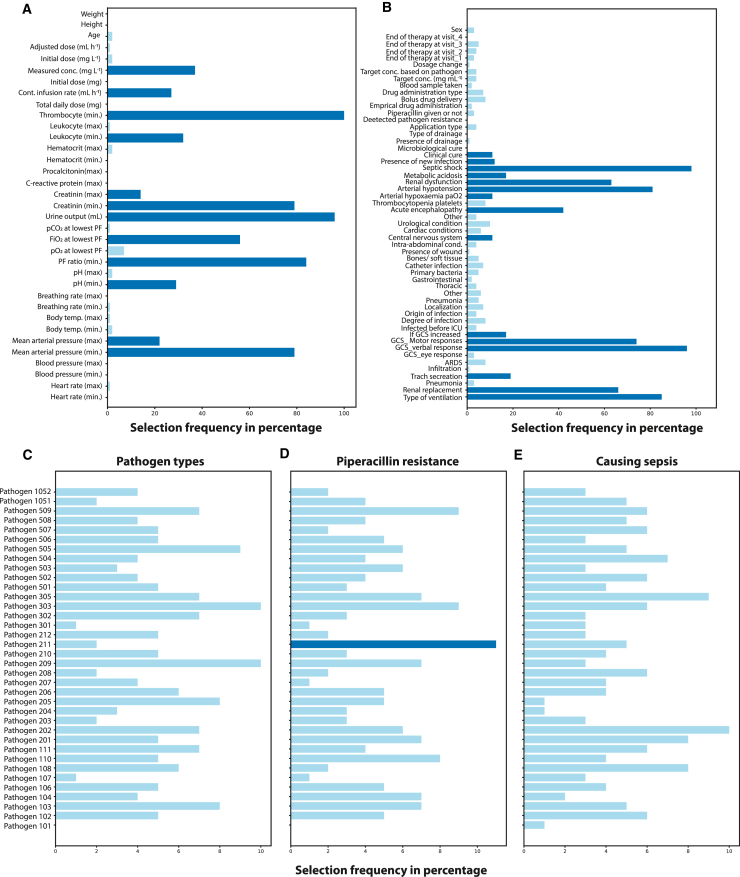
Clinical studies investigating the benefits of beta-lactam therapeutic drug monitoring (TDM) among critically ill patients are hindered by small patient groups, variability between studies, patient heterogeneity, and inadequate use of TDM. Accordingly, definitive conclusions regarding the efficacy of TDM remain elusive. To address these challenges, we propose an innovative approach that leverages data-driven methods to unveil the concealed connections between therapy effectiveness and patient data, collected through a randomized controlled trial (DRKS00011159; 10th October 2016). Our findings reveal that machine learning algorithms can successfully identify informative features that distinguish between healthy and sick states. These hold promise as potential markers for disease classification and severity stratification, as well as offering a continuous and data-driven "multidimensional" Sequential Organ Failure Assessment (SOFA) score. The positive impact of TDM on patient recovery rates is demonstrated by unraveling the intricate connections between therapy effectiveness and clinically relevant data via machine learning.
Keywords: Mahalanobis distance; SOFA score; beta-lactam antibiotics; intensive care unit; machine learning; mathematical similarity; piperacillin/tazobactam; sepsis; septic shock; state space approach; therapeutic drug monitoring.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
References
-
- Williams P.G., Tabah A., Cotta M.O., Sandaradura I., Kanji S., Scheetz M.H., Imani S., Elhadi M., Luque-Pardos S., Schellack N., et al. International survey of antibiotic dosing and monitoring in adult intensive care units. Crit. Care. 2023;27:241–311. doi: 10.1186/S13054-023-04527-1/TABLES/3. - DOI - PMC - PubMed
-
- Hagel S., Bach F., Brenner T., Bracht H., Brinkmann A., Annecke T., Hohn A., Weigand M., Michels G., Kluge S., et al. Effect of therapeutic drug monitoring-based dose optimization of piperacillin/tazobactam on sepsis-related organ dysfunction in patients with sepsis: a randomized controlled trial. Intensive Care Med. 2022;48:311–321. - PMC - PubMed
-
- Adnan S., Li J.X., Wallis S.C., Rudd M., Jarrett P., Paterson D.L., Lipman J., Udy A.A., Roberts J.A. Pharmacokinetics of meropenem and piperacillin in critically ill patients with indwelling surgical drains. Int. J. Antimicrob. Agents. 2013;42:90–93. doi: 10.1016/j.ijantimicag.2013.02.023. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
