

A real-world observation of patients with glioblastoma treated with a personalized peptide vaccine
- PMID: 39127809
- PMCID: PMC11316744
- DOI: 10.1038/s41467-024-51315-8
A real-world observation of patients with glioblastoma treated with a personalized peptide vaccine
Abstract
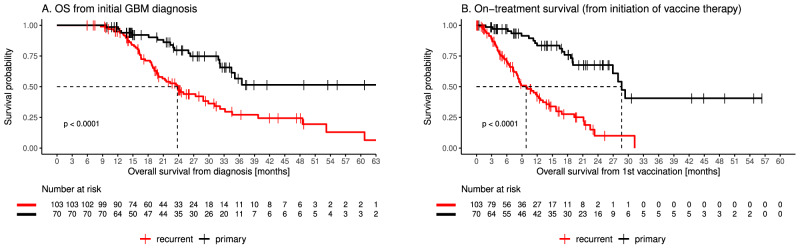
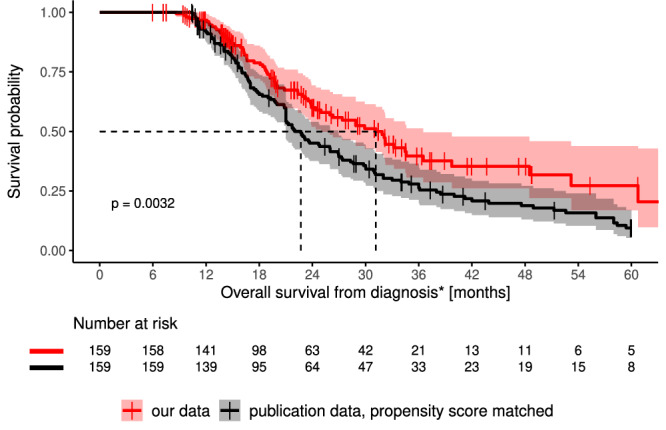
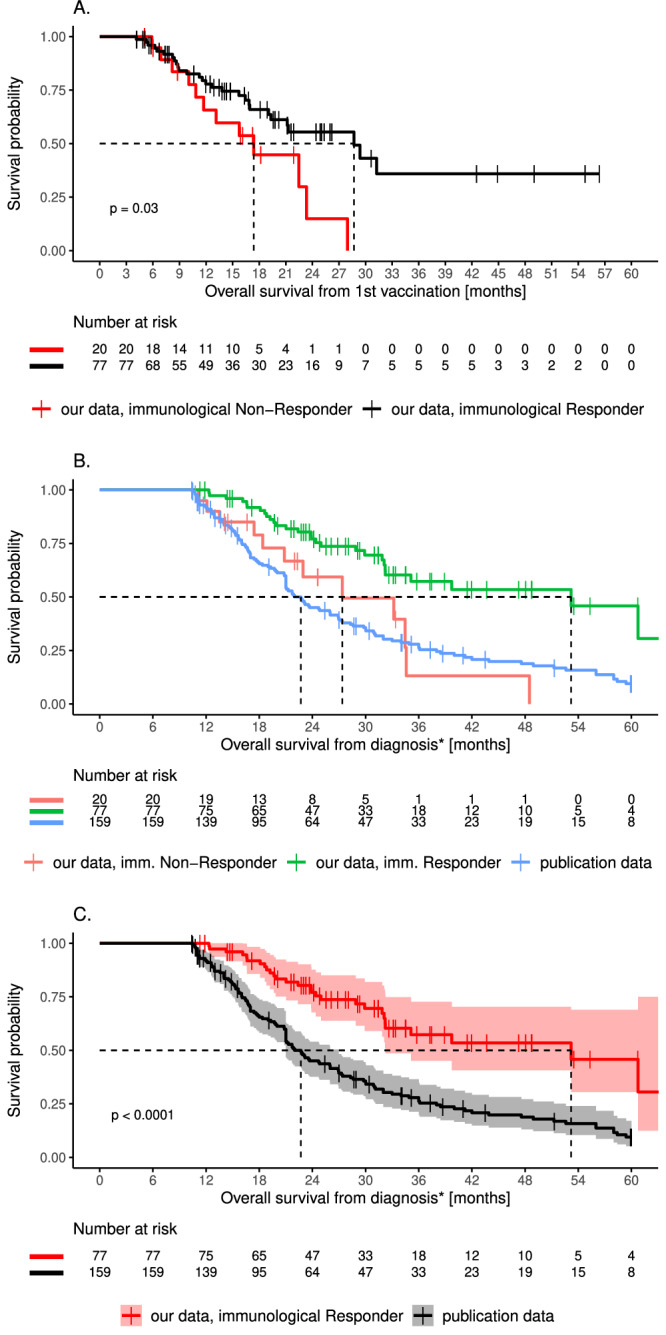
Current treatment outcome of patients with glioblastoma (GBM) remains poor. Following standard therapy, recurrence is universal with limited survival. Tumors from 173 GBM patients are analysed for somatic mutations to generate a personalized peptide vaccine targeting tumor-specific neoantigens. All patients were treated within the scope of an individual healing attempt. Among all vaccinated patients, including 70 treated prior to progression (primary) and 103 treated after progression (recurrent), the median overall survival from first diagnosis is 31.9 months (95% CI: 25.0-36.5). Adverse events are infrequent and are predominantly grade 1 or 2. A vaccine-induced immune response to at least one of the vaccinated peptides is detected in blood samples of 87 of 97 (90%) monitored patients. Vaccine-specific T-cell responses are durable in most patients. Significantly prolonged survival is observed for patients with multiple vaccine-induced T-cell responses (53 months) compared to those with no/low induced responses (27 months; P = 0.03). Altogether, our results highlight that the application of personalized neoantigen-targeting peptide vaccine is feasible and represents a promising potential treatment option for GBM patients.
© 2024. The Author(s).
Conflict of interest statement
Disclosures for Patrick Y. Wen as research support: Astra Zeneca, Black Diamond, Bristol Meyers Squibb, Celgene, Chimerix, Eli Lily, Erasca, Genentech/Roche, Kazia, MediciNova, Merck, Novartis, Nuvation Bio, Servier, Vascular Biogenics, VBI Vaccines. Disclosures for Patrick Y. Wen as advisory board/consultant: Astra Zeneca, Black Diamond, Celularity, Chimerix, Day One Bio, Genenta, Glaxo Smith Kline, Insightec, Kintara, Merck, Mundipharma, Novartis, Novocure, Prelude Therapeutics, Sapience, Servier, Sagimet, Vascular Biogenics, VBI Vaccines. Conflict of interest for Uwe M. Martens as advisory role: BMS, MSD, Roche, Guardant Health, Sanofi-Aventis, GSK, Novartis. Conflict of interest for Uwe M. Martens as scientific support: Dieter Schwarz Foundation. Saskia Biskup and Dirk Biskup have ownership interests in CeCaVa GmbH and CeGaT GmbH. Dirk Hadaschik is an employee of CeCaVa GmbH. Florian Battke, Johannes Harter, and Magdalena Feldhahn are employed by CeGaT GmbH. Alexander Golf, Julian Wünsche, and Thomas Okech are employed by MVZ Zentrum für ambulante Onkologie GmbH. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. No competing interests were disclosed by the other authors.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
