

Intraoperative zero-heat-flux thermometry overestimates nasopharyngeal temperature by 0.39 °C: an observational study in patients undergoing congenital heart surgery
- PMID: 39127818
- PMCID: PMC11821722
- DOI: 10.1007/s10877-024-01204-8
Intraoperative zero-heat-flux thermometry overestimates nasopharyngeal temperature by 0.39 °C: an observational study in patients undergoing congenital heart surgery
Abstract
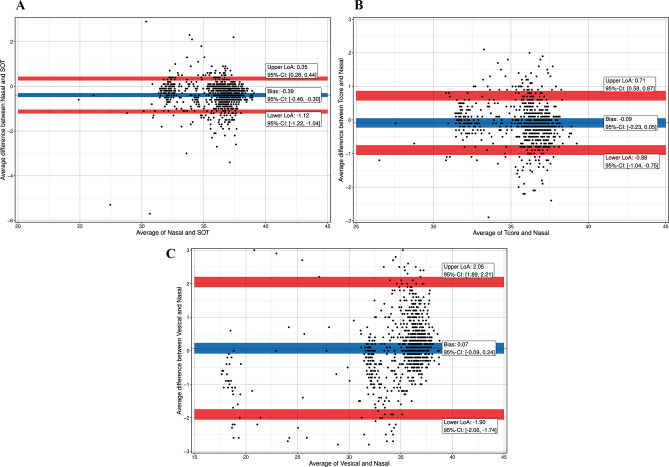
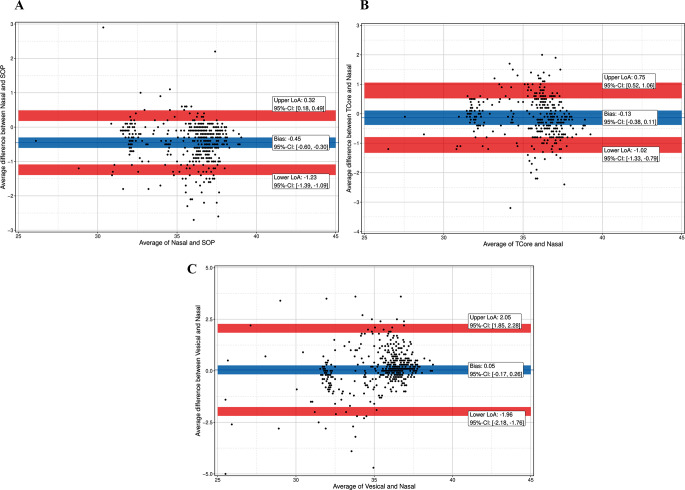
During surgery for congenital heart disease (CHD) temperature management is crucial. Vesical (Tves) and nasopharyngeal (TNPH) temperature are usually measured. Whereas Tves slowly responds to temperature changes, TNPH carries the risk of bleeding. The zero-heat-flux (ZHF) temperature monitoring systems SpotOn™ (TSpotOn), and Tcore™ (Tcore) measure temperature non-invasively. We evaluated accuracy and precision of the non-invasive devices, and of Tves compared to TNPH for estimating temperature. In this prospective observational study in pediatric and adult patients accuracy and precision of TSpotOn, Tcore, and Tves were analyzed using the Bland-Altman method. Proportion of differences (PoD) and Lin´s concordance correlation coefficient (LCC) were calculated. Data of 47 patients resulted in sets of matched measurements: 1073 for TSpotOn vs. TNPH, 874 for Tcore vs. TNPH, and 1102 for Tves vs. TNPH. Accuracy was - 0.39 °C for TSpotOn, -0.09 °C for Tcore, and 0.07 °C for Tves. Precisison was between - 1.12 and 0.35 °C for TSpotOn, -0.88 to 0.71 °C for Tcore, and - 1.90 to 2.05 °C for Tves. PoD ≤ 0.5 °C were 71% for TSpotOn, 71% for Tcore, and 60% for Tves. LCC was 0.9455 for TSpotOn, 0.9510 for Tcore, and 0.9322 for Tves. Temperatures below 25.2 °C (TSpotOn) or 27.1 (Tcore) could not be recorded non-invasively, but only with Tves. Trial registration German Clinical Trials Register, DRKS00010720.
Keywords: Congenital heart disease; Core temperature; Hypothermia; Non-invasive monitoring; Zero-heat-flux thermometer.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This prospective single-center observational study was conducted at the University Medical Centre Göttingen, Germany, after obtaining local ethics committee approval (No. 5/3/16), and registration on the German Clinical Trials Register (DRKS00010720). We followed STROBE guidelines for reporting of observational studies. Consent to participate: Each patient consented to participate at least 24 h prior to surgery. Consent could be withdrawn by every patient at any time without reason and without any disadvantage regarding treatment. Consent to publish: Each patient consented to publish their data prior to data acquisition. Consent could be withdrawn by every patient at any time without reason and without any disadvantage regarding treatment. Competing interests: Prof. Dr. A. Bräuer is a member of the advisory board of 3 M Europe and has received payments from 3 M Germany, 3 M Europe, 3 M Asia Pacific Pte Ltd. for consultancy work.All other authors do not have any competing interests.
Figures


References
-
- Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of wound infection and temperature group. N Engl J Med. 1996;334(19):1209–15. - PubMed
-
- Melling AC, et al. Effects of preoperative warming on the incidence of wound infection after clean surgery: a randomised controlled trial. Lancet. 2001;358(9285):876–80. - PubMed
-
- Schmied H, et al. Mild hypothermia increases blood loss and transfusion requirements during total hip arthroplasty. Lancet. 1996;347(8997):289–92. - PubMed
-
- Frank SM, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA. 1997;277(14):1127–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
