

The utility of urine sodium-guided diuresis during acute decompensated heart failure
- PMID: 39128947
- PMCID: PMC11455821
- DOI: 10.1007/s10741-024-10424-8
The utility of urine sodium-guided diuresis during acute decompensated heart failure
Abstract
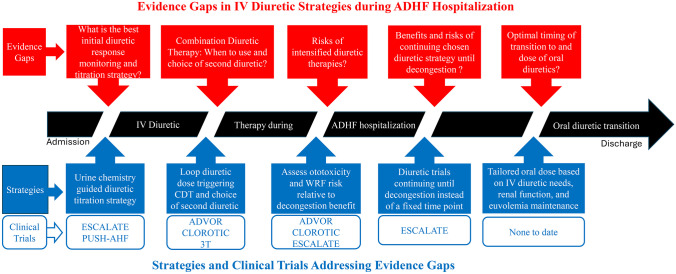
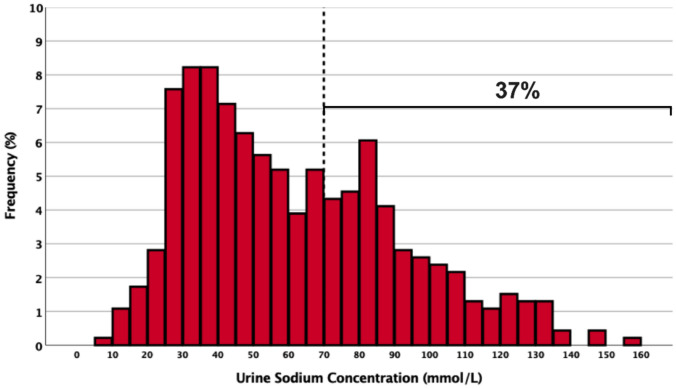
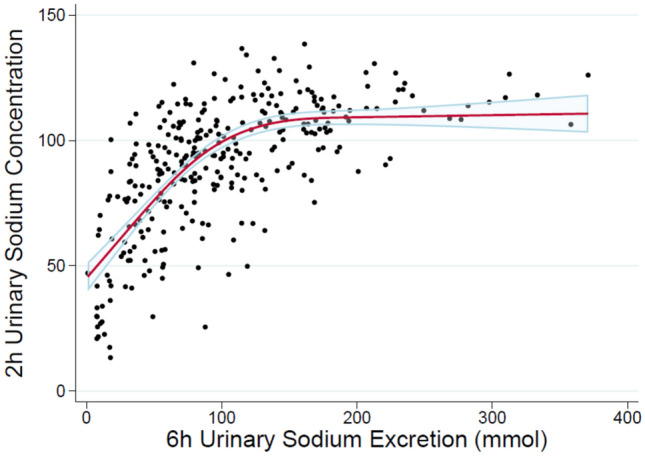
Diuresis to achieve decongestion is a central aim of therapy in patients hospitalized for acute decompensated heart failure (ADHF). While multiple approaches have been tried to achieve adequate decongestion rapidly while minimizing adverse effects, no single diuretic strategy has shown superiority, and there is a paucity of data and guidelines to utilize in making these decisions. Observational cohort studies have shown associations between urine sodium excretion and outcomes after hospitalization for ADHF. Urine chemistries (urine sodium ± urine creatinine) may guide diuretic titration during ADHF, and multiple randomized clinical trials have been designed to compare a strategy of urine chemistry-guided diuresis to usual care. This review will summarize current literature for diuretic monitoring and titration strategies, outline evidence gaps, and describe the recently completed and ongoing clinical trials to address these gaps in patients with ADHF with a particular focus on the utility of urine sodium-guided strategies.
Keywords: Acute decompensated heart failure; Decongestion; Diuresis; Diuretic strategy; Natriuresis; Urine sodium.
© 2024. The Author(s).
Conflict of interest statement
ZC receives research funding from AstraZeneca and consultancy fees from Roche, Lexicon Pharmaceuticals, Abiomed, and Kestra Medical Technologies. KD reports speaker and consultancy fees to institutions from AstraZeneca, Boehringer Ingelheim, and Abbott. JHH receives research funding from the NIA, Boehringer Ingelheim, and Merck. JMTM reports speaker and/or consultancy fees to institutions from Novartis, Boehringer Ingelheim, Moderna, Roche, and Novo Nordisk and receives personal grants from the Netherlands Heart Foundation and Netherlands Organization for Scientific Research (NWO). JL receives research funding from AstraZeneca, Volumetrix, Sensible Medical, and NIH and consulting fees from AstraZeneca, Abbott, Alleviant, Boehringer Ingelheim, Boston Scientific, CVRx, Edwards Lifesciences, Medtronic, Merck, Vascular Dynamics, VWave, and Whiteswell. JT reports grants and/or personal fees from 3ive labs, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Astra Zeneca, Novartis, Cardionomic, MagentaMed, Reprieve Inc., FIRE1, W.L. Gore, Sanofi, Sequana Medical, Otsuka, Abbott, Merck, Windtree Therapeutics, Lexicon Pharmaceuticals, Precardia, Relypsa, Regeneron, BD, Edwards life sciences, and Lilly. In addition, JMT has a patent treatment of diuretic resistance issued to Yale and Corvidia Therapeutics Inc., a patent method for measuring renalase issued to Yale, and a patent treatment of diuretic resistance pending with Reprieve Inc. SPC reports consulting with Boehringer Ingelheim, Aiphia, and Siemens and research support from PCORI, NIH, and Beckman Coulter.
Authors JMTM and KD are Editorial Board Members of the journal.
Figures
References
-
- Heidenreich PA, Bozkurt B, Aguilar D et al (2022) 2022 AHA/ACC/HFSA Guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 10.1161/CIR.0000000000001063.10.1161/CIR.0000000000001063 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
