

Genotype is associated with left ventricular reverse remodelling and early events in recent-onset dilated cardiomyopathy
- PMID: 39129193
- PMCID: PMC11631235
- DOI: 10.1002/ehf2.15009
Genotype is associated with left ventricular reverse remodelling and early events in recent-onset dilated cardiomyopathy
Abstract
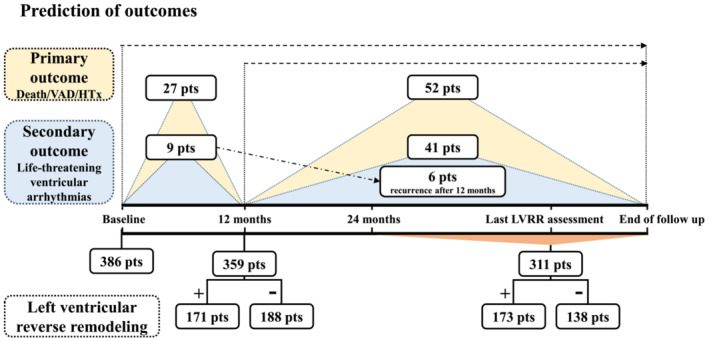
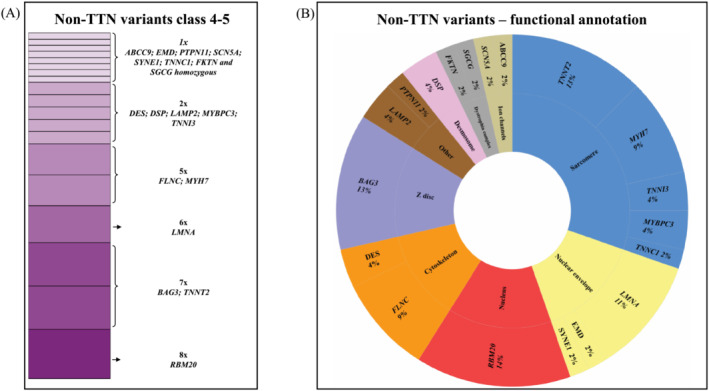
Aims: Recent-onset dilated cardiomyopathy (RODCM) is characterized by heterogeneous aetiology and diverse clinical outcomes, with scarce data on genotype-phenotype correlates. Our aim was to correlate individual RODCM genotypes with left ventricular reverse remodelling (LVRR) and clinical outcomes.
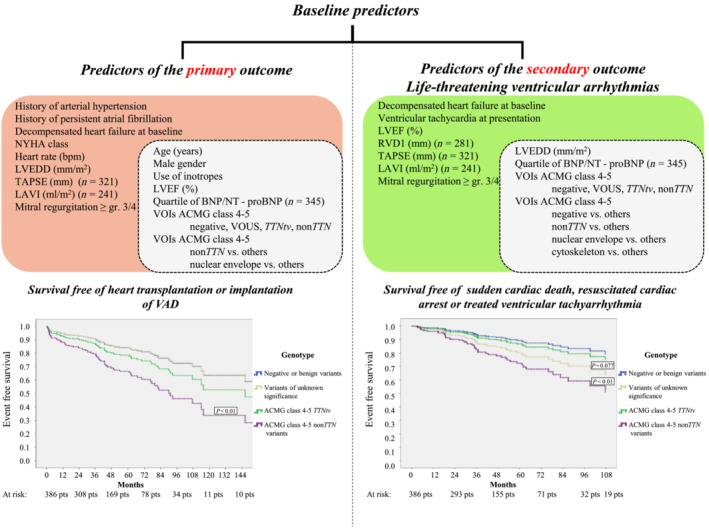
Methods and results: In this prospective study, a total of 386 Czech RODCM patients with symptom duration ≤6 months underwent genetic counselling and whole-exome sequencing (WES). The presence of pathogenic (class 5) or likely pathogenic (class 4) variants in a set of 72 cardiomyopathy-related genes was correlated with the occurrence of all-cause death, heart transplantation, or implantation of a ventricular assist device (primary outcome) and/or ventricular arrhythmia event (secondary outcome). LVRR was defined as an improvement of left ventricular ejection fraction to >50% or ≥10% absolute increase, with a left ventricular end-diastolic diameter ≤33 mm/m2 or ≥10% relative decrease. Median follow-up was 41 months. RODCM was familial in 98 (25%) individuals. Class 4-5 variants of interest (VOIs) were identified in 125 (32%) cases, with 69 (18%) having a single titin-truncating variant (TTNtv) and 56 (14%) having non-titin (non-TTN) VOIs. The presence of class 4-5 non-TTN VOIs, but not of TTNtv, heralded a lower probability of 12-month LVRR and proved to be an independent baseline predictor both of the primary and the secondary outcome. The negative result of genetic testing was a strong protective baseline variable against occurrence of life-threatening ventricular arrhythmias. Detection of class 4-5 VOIs in genes coding nuclear envelope proteins was another independent predictor of both study outcomes at baseline and also of life-threatening ventricular arrhythmias after 12 months. Class 4-5 VOIs of genes coding cytoskeleton were associated with an increased risk of life-threatening ventricular arrhythmias after baseline assessment. A positive family history of dilated cardiomyopathy alone only related to a lower probability of LVRR at 12 months and at the final follow-up.
Conclusions: RODCM patients harbouring class 4-5 non-TTN VOIs are at higher risk of progressive heart failure and life-threatening ventricular arrhythmias. Genotyping may improve their early risk stratification at baseline assessment.
Keywords: Genetics; Left ventricular reverse remodelling; Prognosis; Recent‐onset dilated cardiomyopathy; Whole‐exome sequencing.
© 2024 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
