

Long-term cost-effectiveness of insertion of a biological mesh during stoma-site closure: 5-8-year follow-up of the ROCSS randomized controlled trial
- PMID: 39129618
- PMCID: PMC11317774
- DOI: 10.1093/bjs/znae159
Long-term cost-effectiveness of insertion of a biological mesh during stoma-site closure: 5-8-year follow-up of the ROCSS randomized controlled trial
Abstract
Background: The original ROCSS trial demonstrated a significant reduction in clinically detectable incisional hernias at 2 years in patients receiving prophylactic biological mesh during stoma closure. ROCSS-Ex was designed to investigate the 5-8-year cost-effectiveness of mesh in the surviving cohort using an abdominal wall-specific quality of life score.
Methods: Eligible participants from original UK centres were identified. The primary outcome (abdominal wall-specific quality of life) was measured using the HerQLes score and EQ-5D-5L. Assessors remained blind to patients' original allocation, even if the patient was aware of their treatment.
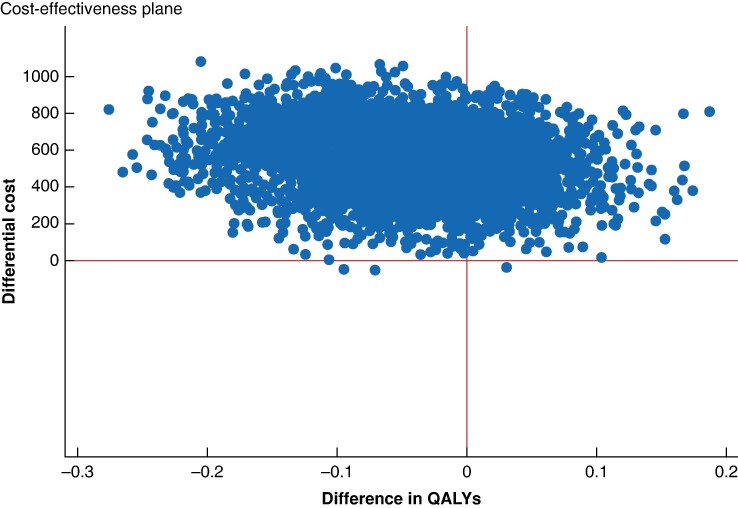
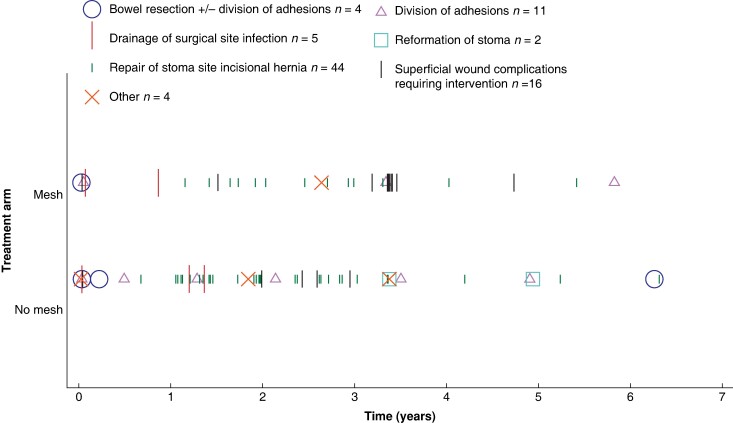
Results: Of the original 790 patients, 598 were available for long-term follow-up. HerQLes scores were available for 396 patients (no mesh: 191, mesh: 205). There was no difference in primary outcome between the two groups (mean difference of 1.48, 95% c.i. (-2.35, 5.32), P = 0.45) and no cost benefit of routine insertion of prophylactic biological mesh across the entire cohort in the long term. However, patients who received mesh experienced significantly fewer stoma site complications within the first 3 years after reversal and needed fewer surgical reinterventions (32 versus 54 for the no mesh group; incidence rate ratio of 0.55, 95% c.i. (0.31, 0.97), P = 0.04).
Conclusions: ROCSS-Ex has shown equivocal outcomes for prophylactic mesh insertion versus standard repair on abdominal wall-specific quality of life 5-8 years after surgery. As most reinterventions occurred within the first 3 years post-surgery, there may be a role for prophylactic mesh in a subset of patients who would be most adversely affected by repeated surgery early on.
Trial registration: ISRCTN25584182 (http://www.clinicaltrials.gov).
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures

References
-
- NHS Digital . Hospital Episode Statistics. 2019. https://digital.nhs.uk/data-and-information/data-tools-and-services/data... (accessed July 2019).
-
- Pokorny H, Herkner H, Jakesz R, Herbst F. Mortality and complications after stoma closure. Arch Surg 2005;140:956–960 - PubMed
-
- Bhangu A, Nepogodiev D, Futaba K; West Midlands Research Collaborative . Systematic review and meta-analysis of the incidence of incisional hernia at the site of stoma closure. World J Surg 2012;36:973–983 - PubMed
-
- Bhangu A, Fletcher L, Kingdon S, Smith E, Nepogodiev D, Janjua U. A clinical and radiological assessment of incisional hernias following closure of temporary stomas. Surgeon 2012;10:321–325 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources