

High-Sensitivity Cardiac Troponin T and Cardiovascular Risk After Ischemic Stroke or Transient Ischemic Attack
- PMID: 39130023
- PMCID: PMC11312770
- DOI: 10.1016/j.jacadv.2024.101022
High-Sensitivity Cardiac Troponin T and Cardiovascular Risk After Ischemic Stroke or Transient Ischemic Attack
Abstract
Background: High-sensitivity cardiac troponin T (hs-cTnT) is associated with cardiovascular disease (CVD) risk in general and various high-risk populations.
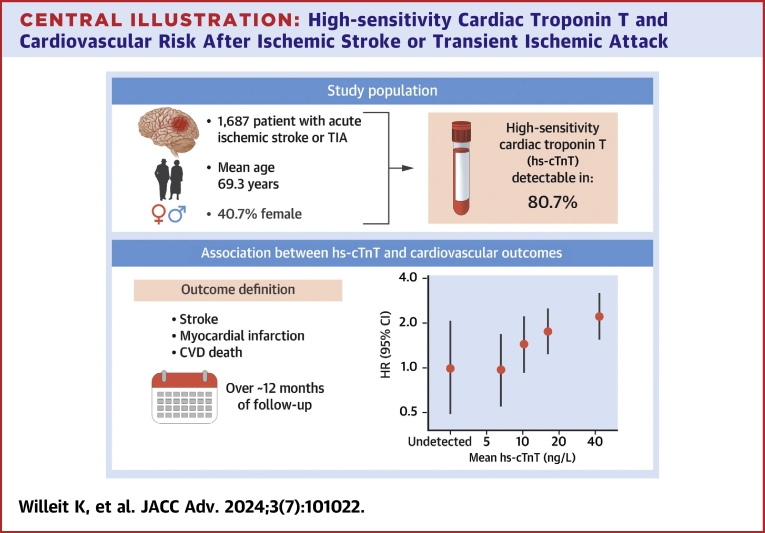
Objectives: The purpose of this study was to precisely characterize the association of hs-cTnT with CVD risk in patients following acute ischemic stroke or transient ischemic attack.
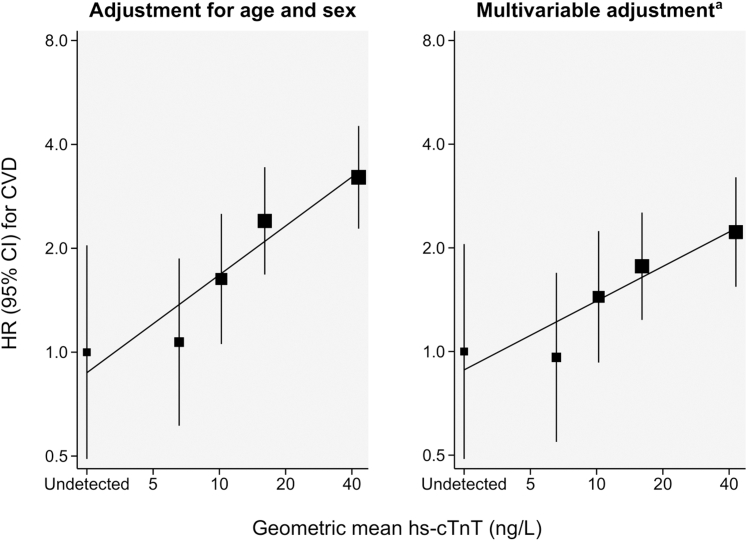
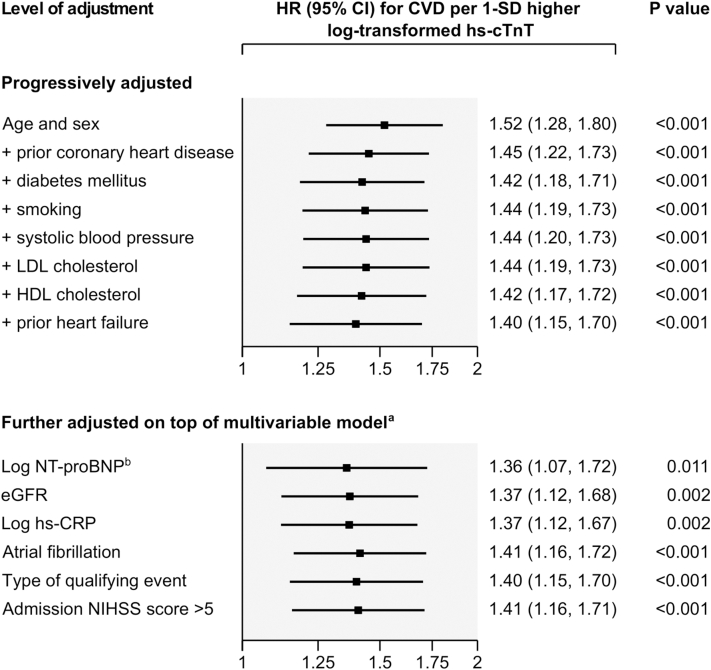
Methods: We conducted post hoc analyses of data from the STROKE-CARD trial (NCT02156778), a pragmatic randomized controlled trial of a disease management program in patients with acute ischemic stroke or transient ischemic attack (ABCD2 score ≥3). We measured hs-cTnT on admission (Roche Elecsys, detection limit 5 ng/L) and quantified HRs for a composite CVD outcome (ie, stroke, myocardial infarction, CVD death) adjusted for age, sex, prior coronary heart disease, prior heart failure, diabetes, smoking, systolic blood pressure, and low- and high-density-lipoprotein cholesterol.
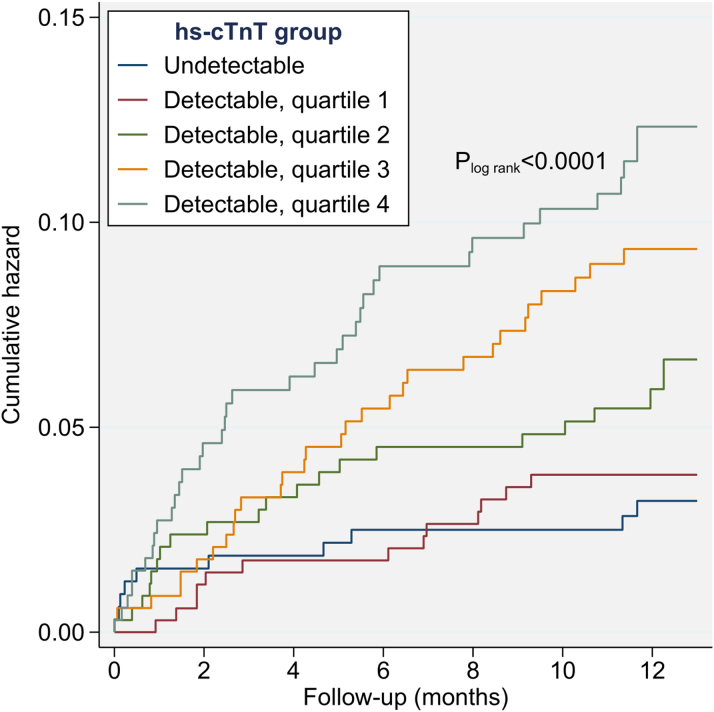
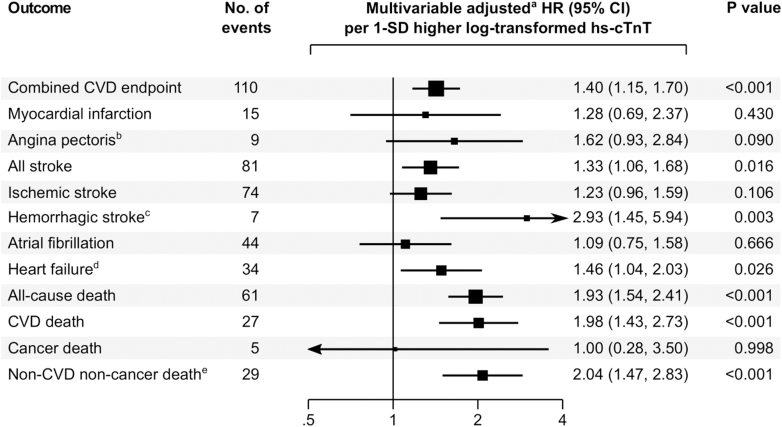
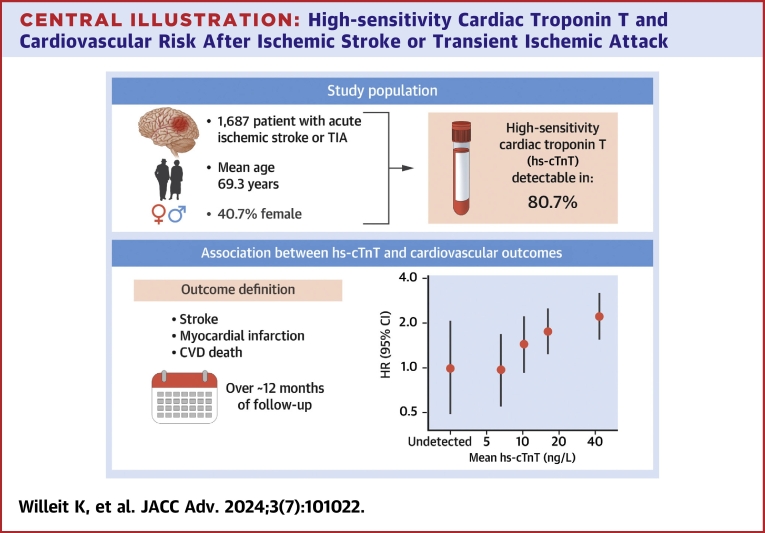
Results: Among 1,687 patients (mean age, 69.3 ± 13.7 years; 40.7% female), hs-cTnT was detectable in 80.7%. Median hs-cTnT was 10 ng/L (IQR: 6-18 ng/L). Over a median follow-up of 12.1 months, 110 patients had a CVD event. The association of hs-cTnT level with CVD risk was of log-linear shape, with a multivariable-adjusted HR of 1.40 (95% CI: 1.15-1.70; P < 0.001) per 1-SD higher log-transformed hs-cTnT value. The strength of association was similar when further adjusted for other potential confounders and across clinically relevant subgroups. Corresponding outcome-specific HRs were 1.33 (95% CI: 1.06-1.68; P = 0.016) for stroke, 1.28 (95% CI: 0.69-2.37; P = 0.430) for myocardial infarction, 1.98 (95% CI: 1.43-2.73; P < 0.001) for CVD death, and 1.93 (95% CI: 1.54-2.41; P < 0.001) for all-cause death.
Conclusions: High hs-cTnT is associated with increased CVD risk in ischemic stroke and transient ischemic attack patients.
Keywords: cardiovascular risk; ischemic stroke; secondary prevention; transient ischemic attack; troponin T.
© 2024 The Authors.
Conflict of interest statement
The STROKE-CARD trial was financially supported by the University Hospital (Tirol Kliniken), Tyrolean Health Insurance Company (TGKK), the Tyrol Health Care Funds (TGF), and unrestricted research grants from Boehringer Ingelheim, Bayer Healthcare, Nstim Services, and Sanofi. Komarek, Lang, Knoflach, and Kiechl were supported by VASCage-Research Centre on Clinical Stroke Research. VASCage is a COMET Centre within the Competence Centers for Excellent Technologies (COMET) program and funded by the Federal Ministry for Climate Action, Environment, Energy, Mobility, Innovation and Technology, the Federal Ministry of Labor and Economy, and the federal states of Tyrol, Salzburg, and Vienna. COMET is managed by the Austrian Research Promotion Agency (Österreichische Forschungsförderungsgesellschaft). FFG Project number: 898252. Prof P. Willeit reports personal fees from Novartis Pharmaceuticals outside the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.PerspectivesCOMPETENCY IN MEDICAL KNOWLEDGE: This study suggests a graded association between elevated high-sensitivity cardiac troponin T concentration and cardiovascular risk in patients after ischemic stroke or transient ischemic attack. TRANSLATIONAL OUTLOOK: Future research is needed to clarify whether patients with elevated high-sensitivity cardiac troponin T benefit from additional targeted preventive measures, including a tailored cardiac workup.
Figures
References
-
- Bergström L., Irewall A.-L., Söderström L., Ögren J., Laurell K., Mooe T. One-year incidence, time trends, and predictors of recurrent ischemic stroke in Sweden from 1998 to 2010: an observational study. Stroke. 2017;48:2046–2051. - PubMed
-
- Sposato L.A., Lam M., Allen B., Shariff S.Z., Saposnik G., PARADISE Study Group First-ever ischemic stroke and incident major adverse cardiovascular events in 93 627 older women and men. Stroke. 2020;51:387–394. - PubMed
-
- Farmakis D., Mueller C., Apple F.S. High-sensitivity cardiac troponin assays for cardiovascular risk stratification in the general population. Eur Heart J. 2020;41:4050–4056. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
