

Characteristics and Management of Patients With Cancer and Atrial Fibrillation: The BLITZ-AF Cancer Registry
- PMID: 39130025
- PMCID: PMC11312304
- DOI: 10.1016/j.jacadv.2024.100991
Characteristics and Management of Patients With Cancer and Atrial Fibrillation: The BLITZ-AF Cancer Registry
Abstract
Background: Atrial fibrillation (AF) is a frequent cardiovascular (CV) comorbidity in cancer.
Objectives: The purpose of this study was to examine clinical characteristics and contemporary management of patients with AF and cancer with a specific focus on antithrombotic treatments.
Methods: This was a prospective, multicenter, observational study of patients with a recent cancer diagnosis and electrocardiographically confirmed AF (the BLITZ-AF Cancer Registry). CHA2DS2VASc scores were calculated for study participants.
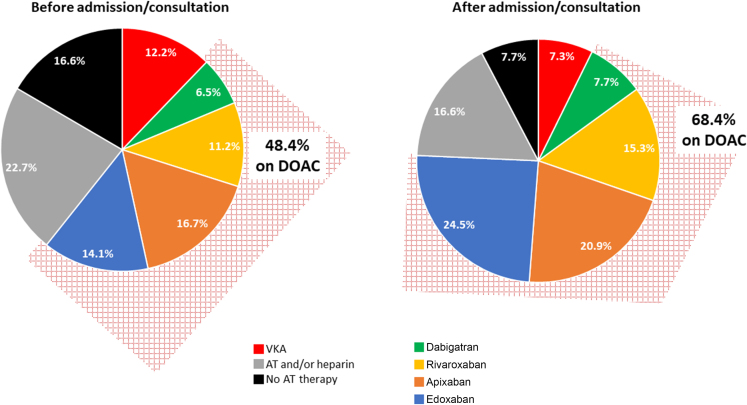
Results: Overall, 1,514 individuals were enrolled from June 2019 to September 2021 (mean age 74 ± 9 years, 47.5% of participants >75 years of age; 63.5% males). CV diseases were common: 20.9% had heart failure, 18.1% had coronary artery disease, 38.5% had valvular heart disease, and 9.8% had peripheral artery disease. Previous thromboembolic and hemorrhagic events occurred in 13.9% and 10.4% of subjects, respectively. The most common cancer types were lung (14.9%), colorectal (14.1%), prostate (8.8%), and non-Hodgkin lymphoma (8.1%). In total, 41.5% of the patients had a CHA2DS2VASc score ≥4. Before admission or prior to cardiologist consultation, 16.6% of subjects were not taking any antithrombotic therapy and 22.7% were receiving antiplatelet agents and/or low-molecular-weight heparin. At discharge or after cardiologic assessment, these percentages dropped to 7.7% and 16.6%, respectively. This trend was paralleled by an increase in the use of direct-acting oral anticoagulant, while the proportion of vitamin K antagonist declined.
Conclusions: This study demonstrates that there is underuse of appropriate antithrombotic therapy for AF in cancer patients highlighting the need to integrate early CV assessment in the management of these patients. (Non-interventional Study on Patients With Atrial Fibrillation and Cancer [BLITZ-AF Cancer]; NCT03909386).
Keywords: antithrombotic; atrial fibrillation; cancer; comorbidities; oral anticoagulants.
© 2024 The Authors.
Conflict of interest statement
The study was realized by Heart Care Foundation with own research funds, partially supported by a not conditional grant by Daiichi Sankyo Italia. Dr Ameri received speaker and/or advisor fees from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Daiichi Sankyo, Janssen, and MSD, all outside the scope of this work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


References
-
- Menichelli D., Vicario T., Ameri P., et al. Cancer and atrial fibrillation: epidemiology, mechanisms, and anticoagulation treatment. Prog Cardiovasc Dis. 2021;66:28–36. - PubMed
-
- Chen S.T., Hellkamp A.S., Becker R.C., et al. Efficacy and safety of rivaroxaban vs warfarin in patients with non-valvular atrial fibrillation and a history of cancer: observations from ROCKET AF. Eur Heart J Qual Care Clin Outcomes. 2019;5:145–152. - PubMed
-
- Pastori D., Marang A., Bisson A., et al. Thromboembolism, mortality, and bleeding in 2,435,541 atrial fibrillation patients with and without cancer: a nationwide cohort study. Cancer. 2021;127:2122–2129. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
