

Not All Patients with a Headache need a CT Scan, but they should be Listened to, and also with a Stethoscope: A Report of a Large Arteriovenous Malformation with a Loud Cranial Bruit
- PMID: 39130073
- PMCID: PMC11313121
- DOI: 10.12890/2024_004669
Not All Patients with a Headache need a CT Scan, but they should be Listened to, and also with a Stethoscope: A Report of a Large Arteriovenous Malformation with a Loud Cranial Bruit
Abstract
Background: Arteriovenous malformations (AVMs) are abnormal direct connections between arterial and venous systems, without an interposed capillary bed. This permits high-flow arteriovenous shunting, which precipitates structural changes in the afferent and efferent vessels, namely arterial smooth muscle hyperplasia and thinning of venous walls. Patients with intracranial AVMs typically present with a haemorrhage, headache or seizure. Treatment is either via medical management aimed at control of seizures, headache and blood pressure, or interventional via surgical, radiation or radiologically guided embolisation.
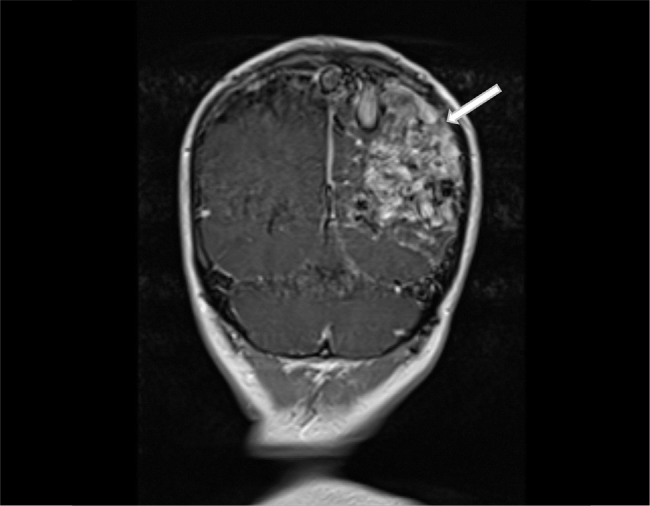
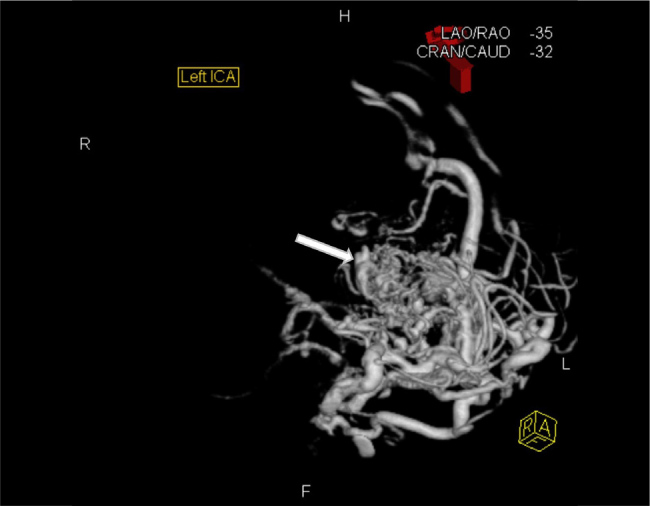
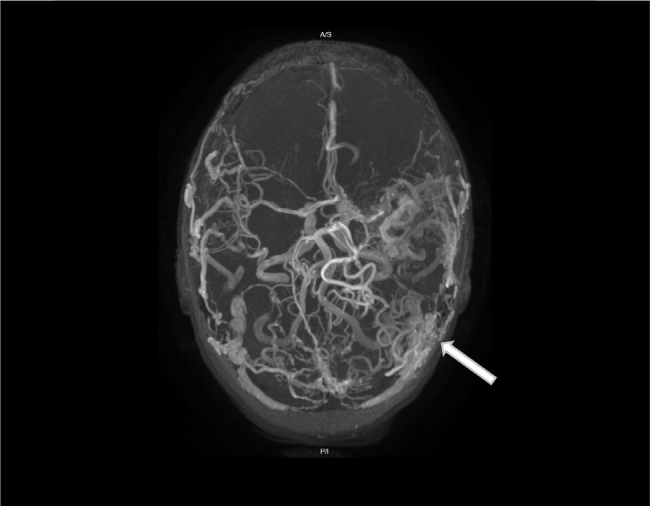
Case description: We report the case of a woman in her early 40s presenting with a tonic-clonic seizure against a background of a 31-year history of migraine and an 18-month history of tremors in her right arm. The clinical examination was remarkable for an extremely loud cranial bruit and a right homonymous hemianopia. Imaging diagnosed an 8 cm Martin-Spetzler grade V intracranial arteriovenous malformation in her left parietal lobe, which was deemed unsuitable for operative or radiotherapy-based intervention.
Conclusion: The patient was managed through observation and relatively good control of her breakthrough seizures was achieved through the addition of brivaracetam to her lamotrigine and carbamazepine-based therapy, six years after her initial presentation.
Learning points: Arteriovenous malformations may go undetected for decades.The presence of a cranial bruit is an important sign and tool in diagnosing an intracranial arteriovenous malformation. The presence of a homonymous hemianopia, of which a patient may be unaware, helps to localise an intracranial lesion.The risks of operative or radiological intervention must be balanced with the risks of haemorrhage or refractory seizure when adopting a strategy for the treatment of an intracranial arteriovenous malformation. Good control of epileptic symptoms in those deemed not suitable for operative or radiological intervention can be achieved by careful titration of anti-seizure medications.
Keywords: Arteriovenous malformation; Martin-Spetzler; cranial bruit; epilepsy; homonymous hemianopia.
© EFIM 2024.
Conflict of interest statement
Conflicts of Interests: The Authors declare that there are no competing interests.
Figures

References
-
- Lawton MT, Rutledge WC, Kim H, Stapf C, Whitehead KJ, Li DY, et al. Brain arteriovenous malformations. Nat Rev Dis Primers. 2015;1:15008. - PubMed
-
- Mohr JP, Parides MK, Stapf C, Moquete E, Moy CS, Overbey JR, et al. International ARUBA investigators. Medical management with or without Interventional therapy for unruptured brain arteriovenous malformations (ARUBA): a multicentre, non-blinded, randomised trial. Lancet. 2014;383:614–621. - PMC - PubMed
-
- Javadpour M, Al-Mahfoudh R, Mitchell PS, Kirollos R. Outcome of microsurgical excision of unruptured brain arteriovenous malformations in ARUBA-eligible patients. Br J Neurosurg. 2016;30:619–622. - PubMed
LinkOut - more resources
Full Text Sources