

Rapid Development of Primary Right Atrial Angiosarcoma
- PMID: 39131000
- PMCID: PMC11315593
- DOI: 10.7759/cureus.64273
Rapid Development of Primary Right Atrial Angiosarcoma
Abstract
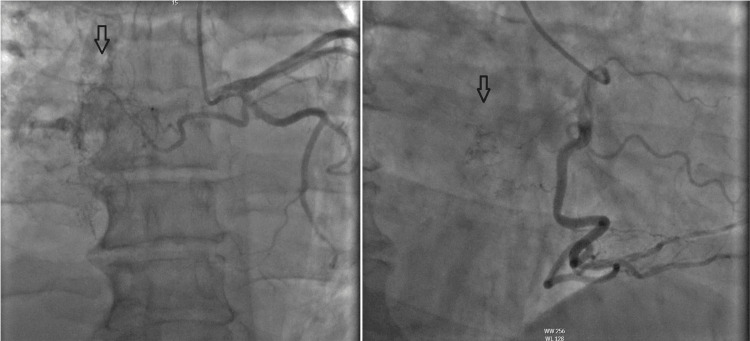
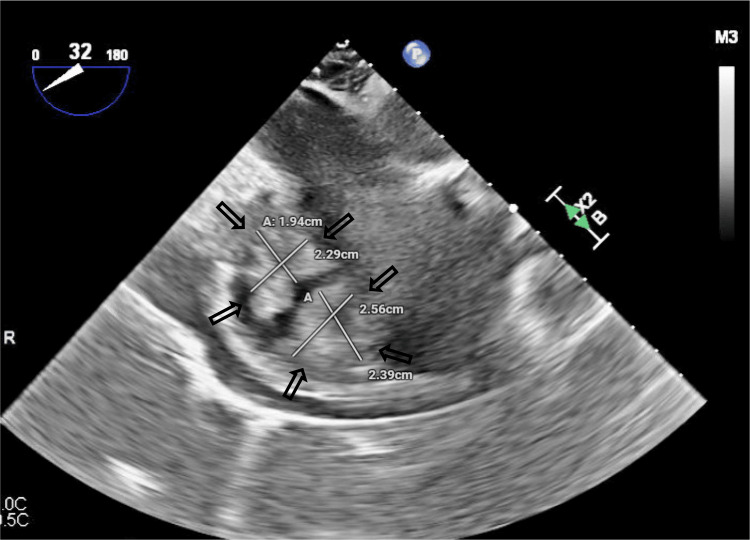
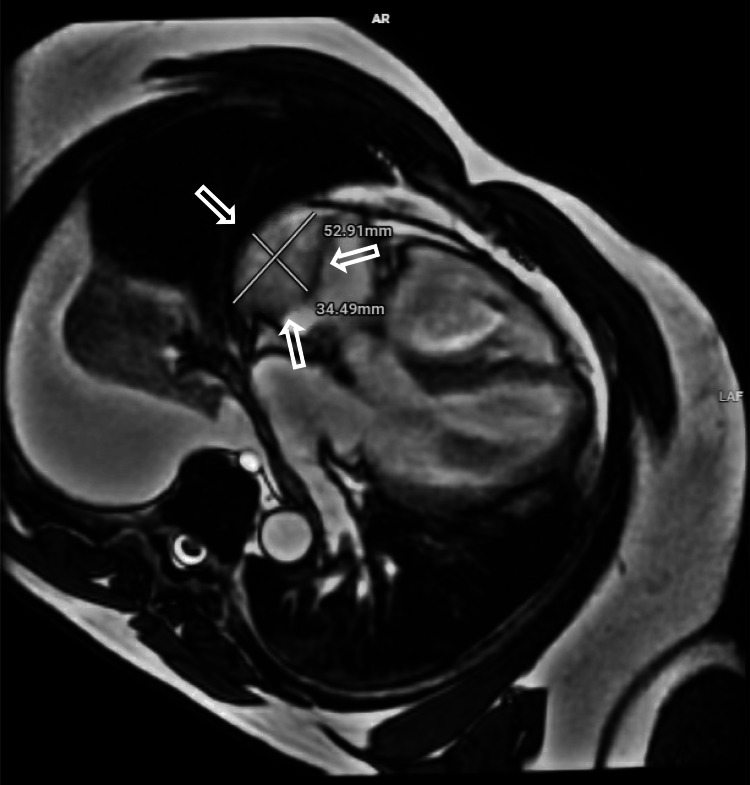
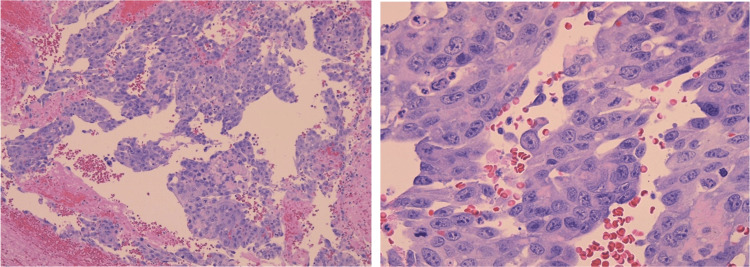
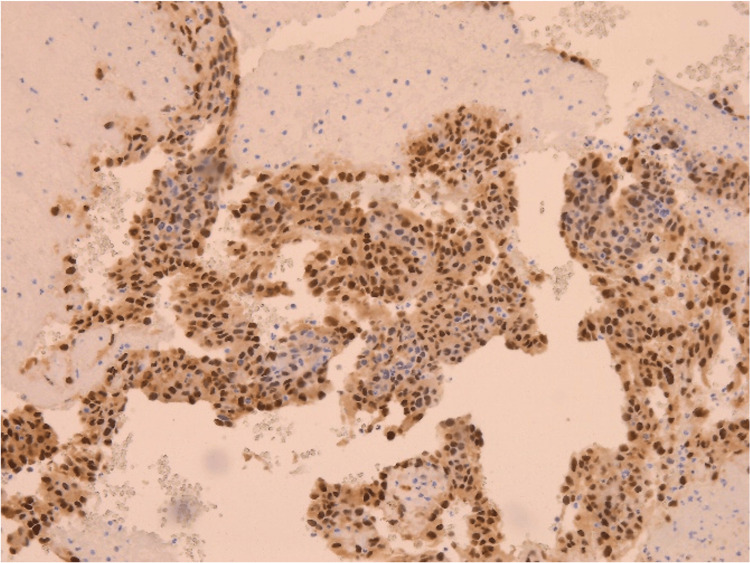
Cardiac angiosarcomas are rare and generally followed by a high level of metastasis with poor median survival outcomes. Echocardiograms, CT scans, and MRIs are the standard methods for finding sites of cardiac tumors; however, immunohistochemical confirmation is necessary for a definitive diagnosis of angiosarcoma. A 58-year-old male presented to the emergency room with one week of dyspnea on moderate exertion accompanied by chest pain and alleviated with rest. A workup done to evaluate mass found a single 5 x 3.5 x 4.8 cm mass heavily vascularized by the right coronary artery and left circumflex involving the free wall of the right atrium with no extension to the tricuspid valve. Surgical resection was performed, and immunohistochemistry was consistent with a primary cardiac angiosarcoma. An exudative fluid analysis on pericardial and pleural fluid analysis may warrant screening for malignancy more frequently in concurrence with a patient's history and presentation. Although the time from onset of symptoms to diagnosis of cardiac angiosarcoma is not well established, further investigation of such correlation may offer insight into survival post-treatment.
Keywords: cardiac angiosarcoma; cardiac tamponade; exudative fluid analysis; pericardial effusion; primary cardiac tumor; transesophageal echocardiogram.
Copyright © 2024, Talbot et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Successful surgical treatment for primary cardiac angiosarcoma: a case report.Gen Thorac Cardiovasc Surg Cases. 2023 Nov 15;2(1):94. doi: 10.1186/s44215-023-00119-1. Gen Thorac Cardiovasc Surg Cases. 2023. PMID: 39516966 Free PMC article.
-
Early Diagnosis of Primary Right Atrial Angiosarcoma From Intraoperative Transesophageal Echocardiographic Findings of Right Atrial Pseudoaneurysm and Cardiac Rupture.Cureus. 2024 Nov 12;16(11):e73521. doi: 10.7759/cureus.73521. eCollection 2024 Nov. Cureus. 2024. PMID: 39534546 Free PMC article.
-
Resection of primary cardiac angiosarcoma infiltrating the right atrioventricular junction and tricuspid valve: a case report.J Cardiothorac Surg. 2021 Mar 21;16(1):41. doi: 10.1186/s13019-021-01426-w. J Cardiothorac Surg. 2021. PMID: 33743733 Free PMC article.
-
Right atrial epithelioid angiosarcoma with multiple pulmonary metastasis confirmed by multimodality imaging-guided pulmonary biopsy: A case report and literature review.Medicine (Baltimore). 2018 Jul;97(30):e11588. doi: 10.1097/MD.0000000000011588. Medicine (Baltimore). 2018. PMID: 30045289 Free PMC article. Review.
-
Spindle cell sarcoma of the right atrium causing right atrial pseudoaneurysm: a case report and review of the literature.J Cardiothorac Surg. 2021 Mar 19;16(1):27. doi: 10.1186/s13019-021-01404-2. J Cardiothorac Surg. 2021. PMID: 33741020 Free PMC article. Review.
References
-
- Angiosarcoma: a review of diagnosis and current treatment. Cao J, Wang J, He C, Fang M. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6895451/ Am J Cancer Res. 2019;9:2303–2313. - PMC - PubMed
-
- Outcomes after surgical resection of cardiac sarcoma in the multimodality treatment era. Bakaeen FG, Jaroszewski DE, Rice DC, et al. J Thorac Cardiovasc Surg. 2009;137:1454–1460. - PubMed
-
- Cutaneous soft tissue sarcoma incidence patterns in the U.S.: an analysis of 12,114 cases. Rouhani P, Fletcher CD, Devesa SS, Toro JR. Cancer. 2008;113:616–627. - PubMed
-
- Characteristics and survival of malignant cardiac tumors: a 40-year analysis of >500 patients. Oliveira GH, Al-Kindi SG, Hoimes C, Park SJ. Circulation. 2015;132:2395–2402. - PubMed
-
- Angiosarcoma. Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ. Lancet Oncol. 2010;11:983–991. - PubMed
Publication types
LinkOut - more resources
Full Text Sources