

Primary Central Nervous System Vasculitis Mimicking Susac Syndrome and Multiple Sclerosis With Long-Term Remission and Spontaneous Resolution of Lesions: A Case Report
- PMID: 39131025
- PMCID: PMC11316671
- DOI: 10.7759/cureus.64358
Primary Central Nervous System Vasculitis Mimicking Susac Syndrome and Multiple Sclerosis With Long-Term Remission and Spontaneous Resolution of Lesions: A Case Report
Abstract
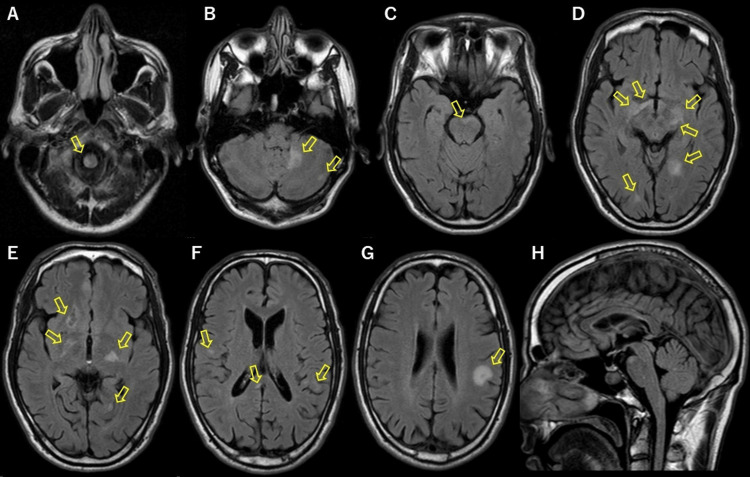
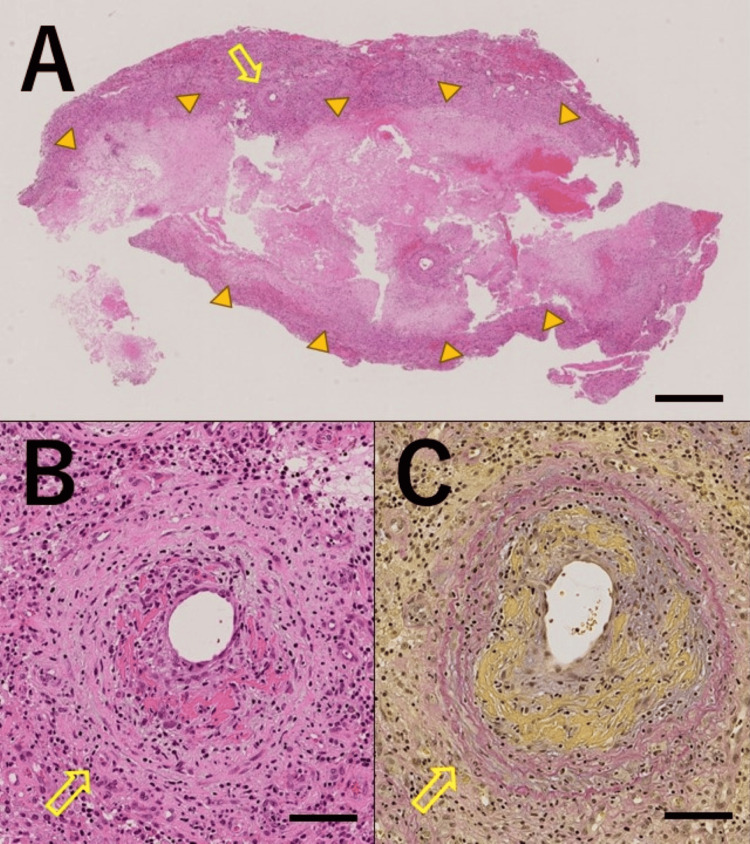
Primary central nervous system vasculitis (PCNSV) is an angiitis localized to the central nervous system (CNS), with various manifestations and no specific biomarkers. Herein, we report a case of PCNSV that presented with an unusual course. A 40-year-old Japanese male developed inner ear symptoms and visual field disturbances. Later, at 42 years of age, the patient developed right hemiparesis and was diagnosed with multiple sclerosis (MS). He received methylprednisolone pulse therapy, which improved his symptoms and resolved most brain lesions. Subsequently, he did not visit the hospital for 13 years, during which time he experienced no relapse. At 55 years of age, he presented to our hospital with fatigue and dizziness. Susac syndrome was suspected because of sensorineural hearing loss and snowball lesions in the corpus callosum. Some of the brain lesions resolved spontaneously. A biopsy was performed on a right frontal lobe lesion, which revealed vasculitis with fibrinoid necrosis, no demyelinating lesions, no amyloid positivity, and no infiltration of atypical lymphocytes. With no evidence of vasculitis in other organs, the patient was diagnosed with PCNSV. The patient was treated with methylprednisolone pulse therapy, followed by oral prednisolone (1 mg/kg/day). The prednisolone was tapered off, and no relapse of symptoms or new lesions on magnetic resonance imaging (MRI) were noted. As observed in this case, even in a scenario suggestive of Susac syndrome or multiple sclerosis, PCNSV should be considered a differential diagnosis and confirmed via brain biopsy.
Keywords: biopsy; central nervous system vasculitis; long-term remission; multiple sclerosis; spontaneous resolution of lesions; susac syndrome.
Copyright © 2024, Koseki et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Primary central nervous system vasculitis - an update on diagnosis, differential diagnosis and treatment. Kraemer M, Berlit P. J Neurol Sci. 2021;424:117422. - PubMed
-
- Relapse rates and long-term outcome in primary angiitis of the central nervous system. Schuster S, Ozga AK, Stellmann JP, et al. J Neurol. 2019;266:1481–1489. - PubMed
-
- Adult primary angiitis of the central nervous system: isolated small-vessel vasculitis represents distinct disease pattern. de Boysson H, Boulouis G, Aouba A, et al. Rheumatology (Oxford) 2017;56:439–444. - PubMed
-
- Primary angiitis of the central nervous system: emerging variants. MacLaren K, Gillespie J, Shrestha S, Neary D, Ballardie FW. QJM. 2005;98:643–654. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials