

Association Between Low-Dose Ketamine After Periacetabular and/or Femoral Osteotomy and Postoperative Opioid Requirements
- PMID: 39131097
- PMCID: PMC11311170
- DOI: 10.1177/23259671241257260
Association Between Low-Dose Ketamine After Periacetabular and/or Femoral Osteotomy and Postoperative Opioid Requirements
Abstract
Background: Previous studies have sought to determine the effect of inpatient ketamine therapy on postoperative pain in a variety of surgical specialties.
Purpose: To determine the effects of postoperative ketamine analgesia after periacetabular osteotomy (PAO) and/or derotational femoral osteotomy (DFO) on opioid requirements, pain, and discharge time.
Study design: Cohort study; Level of evidence, 3.
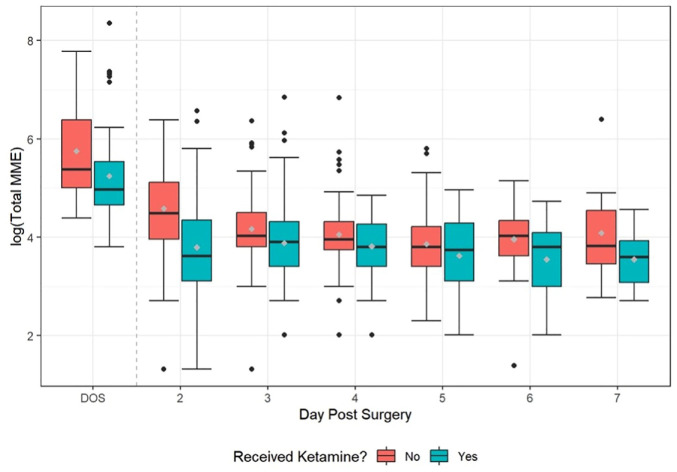
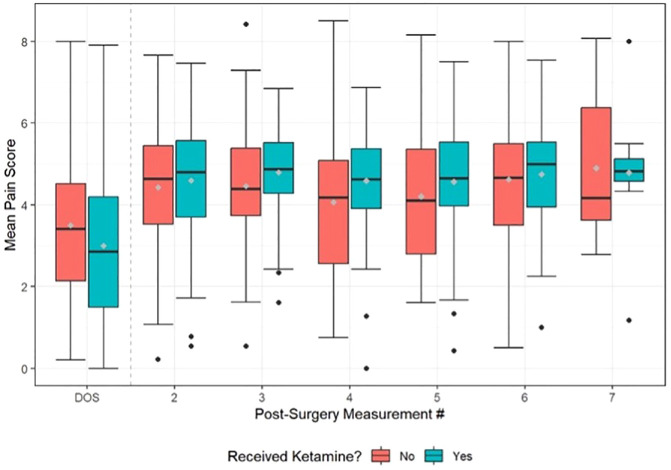
Methods: Prospective data were collected on 145 patients who underwent PAO and/or DFO by the senior author between January 2021 and December 2022. Hip arthroscopy was performed 3 to 10 days before addressing any intra-articular pathology. In 2021, patients (n = 91 procedures; control group) received a traditional postoperative multimodal pain regimen. In 2022, postoperative low-dose ketamine (0.1-1 mg/kg/h) was added to the multimodal analgesic approach until 24 hours before discharge (n = 81 procedures; ketamine group). The ketamine and control groups were matched based on procedure type. Total opioid consumption was collected using milligram morphine equivalents (MMEs) for both groups. Postoperative pain was measured using the Defense and Veterans Pain Rating Scale (DVPRS), which was analyzed as the mean score per day. Data on the mean MME and DVPRS were analyzed for up to 7 days postoperatively. Linear mixed statistical analysis was performed to determine the significance of low-dose postoperative ketamine on postoperative pain and opioid utilization.
Results: Patients who did not receive ketamine after PAO and/or DFO utilized a mean of 181 ± 335 MMEs and had a mean DVPRS score of 4.18 ± 1.63. Patients who received postoperative ketamine required a mean of 119 ± 291 MMEs and had a mean DVPRS score of 4.34 ± 1.61. The ketamine group was found to consume a significantly lower total MME dose per day (P < .001). No significant difference was found in the mean DVPRS score between the ketamine and control groups (P = .42). Also, no significant difference was found on the day of discharge (P = .79).
Conclusion: Patients who received postoperative ketamine after PAO and/or DFO had a significant decrease in MME dose when compared with a control group of patients who did not receive ketamine. Surgeons should consider adding ketamine to their postoperative multimodal pain control protocol to decrease opioid consumption while adequately addressing postoperative pain.
Keywords: ketamine; morphine milligram equivalent; opioids; periacetabular osteotomy; postoperative pain.
© The Author(s) 2024.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: C.Z. owns stock or stock options in AbbVie. O.M.D. holds stock or stock options in HeapSi and MITA and receives IP royalties from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from the University of Colorado Denver (ref No. CRV006-1).
Figures
References
-
- Bell RF, Dahl JB, Moore RA, Kalso E. Peri-operative ketamine for acute post-operative pain: a quantitative and qualitative systematic review (Cochrane review). Acta Anaesthesiol Scand. 2005;49(10):1405-1428. - PubMed
-
- Benyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician. 2008;11(suppl 2):S105-S120. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
