

Immune Checkpoint Inhibitor-Induced Pancreatic Injury: Clinical and Radiological Profile and Response to Steroids
- PMID: 39131139
- PMCID: PMC11308033
- DOI: 10.1016/j.gastha.2023.11.020
Immune Checkpoint Inhibitor-Induced Pancreatic Injury: Clinical and Radiological Profile and Response to Steroids
Abstract
Background and aims: Immune checkpoint inhibitor therapy causes numerous immune-related adverse events, including autoimmune pancreatic injury (AIPI), which results in rapid organ atrophy. We profiled the clinico-radiological features, short-term natural history, and response to steroids of AIPI.
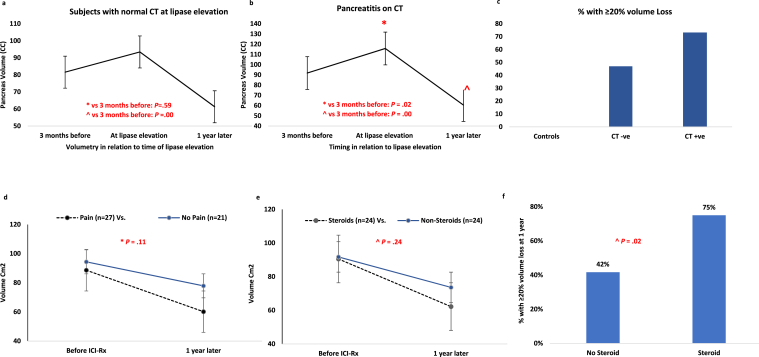
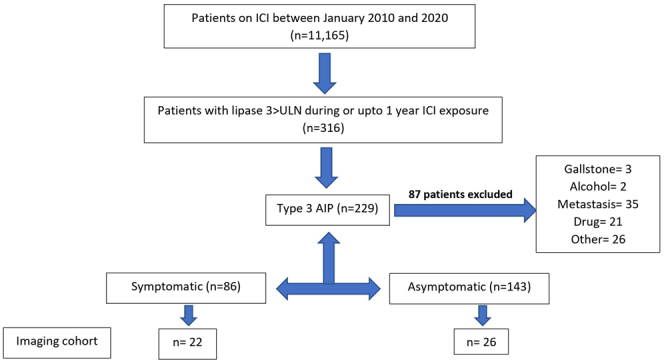
Methods: We retrospectively reviewed medical records of 229/11,165 (2.1%) adult patients with AIPI. One hundred and ten out of 229 (48%) had abdominal computerized tomography (CT) scan at lipase elevation; data of 110 without pancreatic metastases were analyzed. We analyzed serial CT-based pancreas volumetry data in 48 patients with AIPI (32 with normal CT and 16 with pancreatitis on CT at lipase elevation). We examined impact of steroids on pain and disease course.
Results: In AIPI (n = 229), median lipase elevation was 4x upper limit of normal (range: 3-40x). The injury was more often asymptomatic than painful (143/229 (62%) vs 86/229 (38%), P < .000). Majority (83/110 (75%) had normal CT, often in painless vs painful disease: 51/57 (90%) vs 32/53 (60%), P < .001) 25% had interstitial pancreatitis. On serial pancreas volumetry, marked volume (cc) loss occurred 1 year after vs 3 months before lipase elevation in both normal CT (median 81.6 vs 61.3, P = .00) and pancreatitis on CT groups (91.8 vs 60.5, P = .00), ≥20% volume loss occurred in 47% vs 73%, respectively (P = .08). Steroids, when used did not mitigate pain, biochemical relapse, pancreas volume loss or 1-year diabetes incidence (7.2%).
Conclusion: Autoimmune pancreatic injury (AIPI) is uniquely characterized by painless lipase elevation, normal pancreas on CT and rapid pancreatic volume loss on follow-up. Steroids do not appear to have a role in management.
Keywords: CTLA-4; Chronic Pancreatitis; Immune-Related Adverse Events; PD-L1; Pancreatic Atrophy; Steroids; Type 3 AIP.
© 2024 The Authors.
Figures

References
-
- Sury K., Perazella M.A., Shirali A.C. Cardiorenal complications of immune checkpoint inhibitors. Nat Rev Nephrol. 2018;14:571–588. - PubMed
-
- Sayed Ahmed A., Abreo M., Thomas A., et al. Type 3 autoimmune pancreatitis (immune checkpoint inhibitor-induced pancreatitis) Curr Opin Gastroenterol. 2022;38:516–520. - PubMed
-
- Chari S.T., Kloeppel G., Zhang L., et al. Histopathologic and clinical subtypes of autoimmune pancreatitis: the honolulu consensus document. Pancreatology. 2010;10(6):664–672. - PubMed
-
- Shirwaikar Thomas A., Wang Y. In: Managing immunotherapy related organ toxicities: a practical guide. Wang Y., editor. Springer International Publishing; Cham: 2022. Gastroenterology (GI) pp. 81–96.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
