

Utility of Artificial Intelligence Plaque Quantification: Results of the DECODE Study
- PMID: 39131216
- PMCID: PMC11308844
- DOI: 10.1016/j.jscai.2024.101296
Utility of Artificial Intelligence Plaque Quantification: Results of the DECODE Study
Erratum in
-
Correction.J Soc Cardiovasc Angiogr Interv. 2025 Aug 9;4(10Part A):103930. doi: 10.1016/j.jscai.2025.103930. eCollection 2025 Oct. J Soc Cardiovasc Angiogr Interv. 2025. PMID: 41268087 Free PMC article.
Abstract
Background: Artificial Intelligence Plaque Analysis (AI-QCPA, HeartFlow) provides, from a CCTA, quantitative plaque burden information including total plaque and plaque subtype volumes. We sought to evaluate the clinical utility of AI-QCPA in clinical decision making.
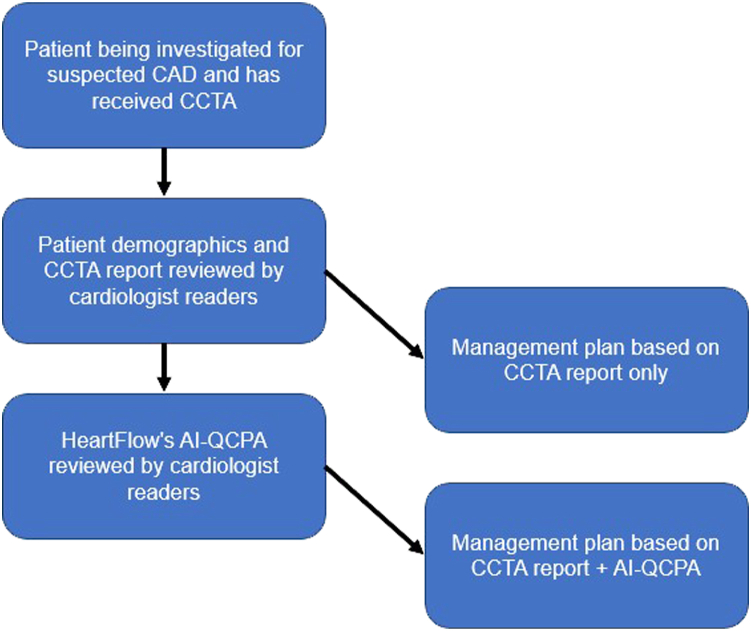
Methods: One hundred cases were reviewed by 3 highly experienced practicing cardiologists who are SCCT level 3 CCTA readers. Patients had varying levels of calcium (median CACS: 99.5) and CAD-RADS scores. Initial management plan for each case was a majority decision based upon patient demographics, clinical history, and CCTA report. AI-QCPA was then provided for each patient, and the plan was reconsidered. The primary endpoint was the reclassification rate (RR). In a secondary analysis of 40 cases, the above process was repeated but the initial plan was based upon review of the actual CCTA images.
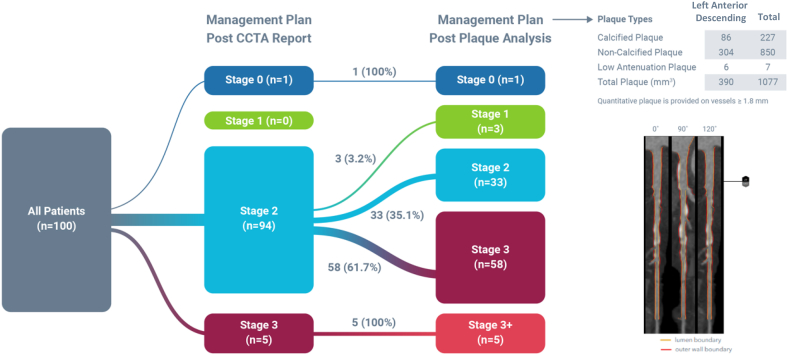
Results: RR following AI-QCPA review was 66% (66/100) of cases (95% CI, 56.72%-75.28%). RR ranged from 47% in cases with CACS 0 to 96% in cases with CACS >400, and from 40% in CAD-RADS 1 cases to 94% in CAD-RADS 4 cases. RR was higher in cases with coronary stenoses ≥50% (89.5%) vs cases with stenoses <50% (51.6%). RR was 39% in cases with LDL <70 mg/dL vs 70% in LDL ≥70 mg/dL. Following review of the CCTA images rather than the CCTA report, the RR was 50% (95% CI of 34.51% - 65.49%). The primary reclassification effect was to intensify preventative medical therapy.
Conclusions: Adding AI-QCPA to CCTA alone leads to a change in clinical care in two-thirds of patients.
Keywords: artificial intelligence quantified coronary plaque analysis; atherosclerosis; coronary artery disease; coronary computed tomographic angiography; coronary plaque; coronary plaque quantification.
Figures
References
-
- Narula J., Stuckey T., Nakazawa G., et al. Primary results of the REVEALPLAQUE study: A prospective quantitative assessment of AI-based CCTA plaque volume compared with IVUS. JCCT. 2023;17(4) doi: 10.1016/j.jcct.2023.05.096. - DOI
-
- Petersen K., Schaap M., Mirza S., et al. Quantitative assessment of AI-based CCTA plaque volume compared with IVUS. J Cardiovasc Comput Tomogr. 2022;16(4 Suppl):S24. doi: 10.1016/j.jcct.2022.06.057. - DOI
-
- Dundas, et al. Interaction of AI-enabled quantitative coronary plaque volumes on coronary CT angiography, FFRCT, and clinical outcomes: a retrospective analysis of the ADVANCE registry. Circ Cardiovasc Imaging. In press. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
